Northwestern University Feinberg School of Medicine
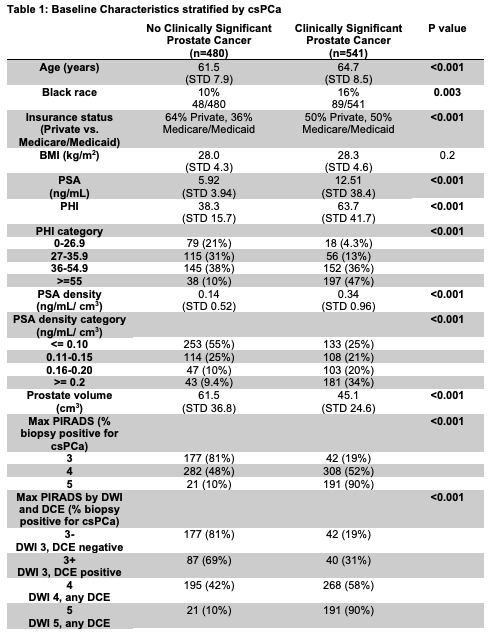
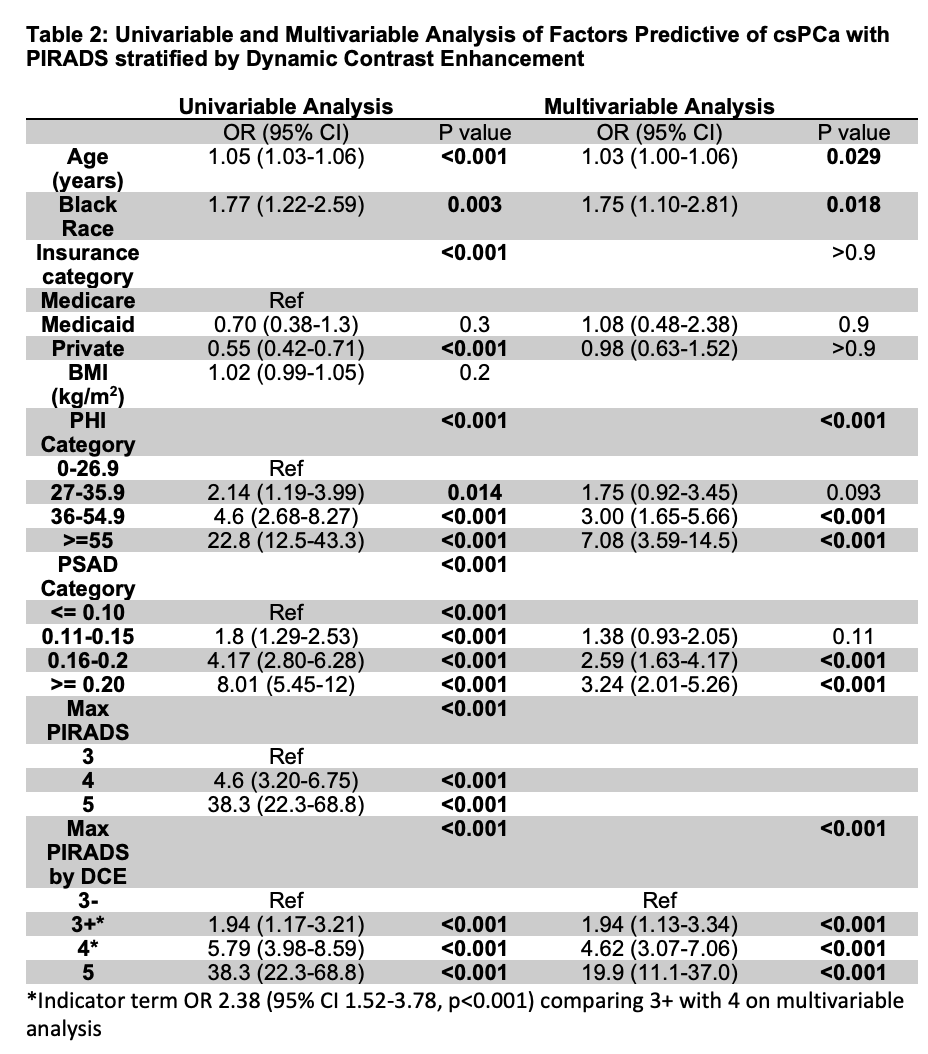
Introduction: Positive dynamic contrast enhancement (DCE) on multiparametric prostate MRI (mpMRI) upgrades peripheral zone (PZ) lesions on diffusion weighted imaging (DWI) from PIRADS 3 to 4, whereas these lesions would remain PIRADS 3 for biparametric MRI. It remains unclear if the rate of clinically significant prostate cancer (csPCa, Gleason Grade Group [GG] =2) differs for patients with DCE upgraded lesions (3+) compared to lesions rated 3 by DWI with negative DCE (3-), or 4 by DWI. Methods: Biopsy naïve men presenting with elevated PSA and pre-biopsy MRI from 2018-2022 were identified. Clinicopathologic and MRI data including highest PIRADS lesion and scoring in individual MRI series were obtained. Patients with PIRADS 1 or 2 or transitional zone lesions as their highest PIRADS lesion were excluded. Patients with multiple lesions were included, and categorized by their highest PIRADS lesion. T-test, Chi-squared, and multivariable logistic regression were performed. Results: 2468 men underwent mpMRI, and 1021 patients who underwent prostate biopsy had PZ lesions as their highest PIRADS lesion. csPCa detection rates for PIRADS 3-, 3+ and 4 were 19%, 31%, and 58%, respectively (p=0.01 for 3- vs 3+; p<0.001 for 3+ vs 4). On multivariable analysis, older age, Black race, PHI >36, PSAD >0.16, and highest PIRADS were significant predictors of csPCa. There was a significant difference in csPCa detection comparing 3+ to 3- (OR 1.94, 95% CI 1.13-3.34, p<0.001) and comparing 4 to 3+ (OR 2.38, 95% CI 1.52-3.78, p<0.001). AUCs for csPCa detection were similar for models classifying patients based on biparametric or multiparametric interpretation of PIRADS (82.0% vs. 81.9%). Conclusions: Patients with PZ lesions upgraded from PIRADS 3 to 4 by DCE have a csPCa detection rate that is higher than those rated as DWI 3 with negative DCE, but lower than those rated as DWI 4. Overall discrimination for biparametric and multiparametric MRI were similar, but DCE findings may aid in individualized cancer risk-stratification and diagnostic decisions. SOURCE OF Funding: None

 photo")