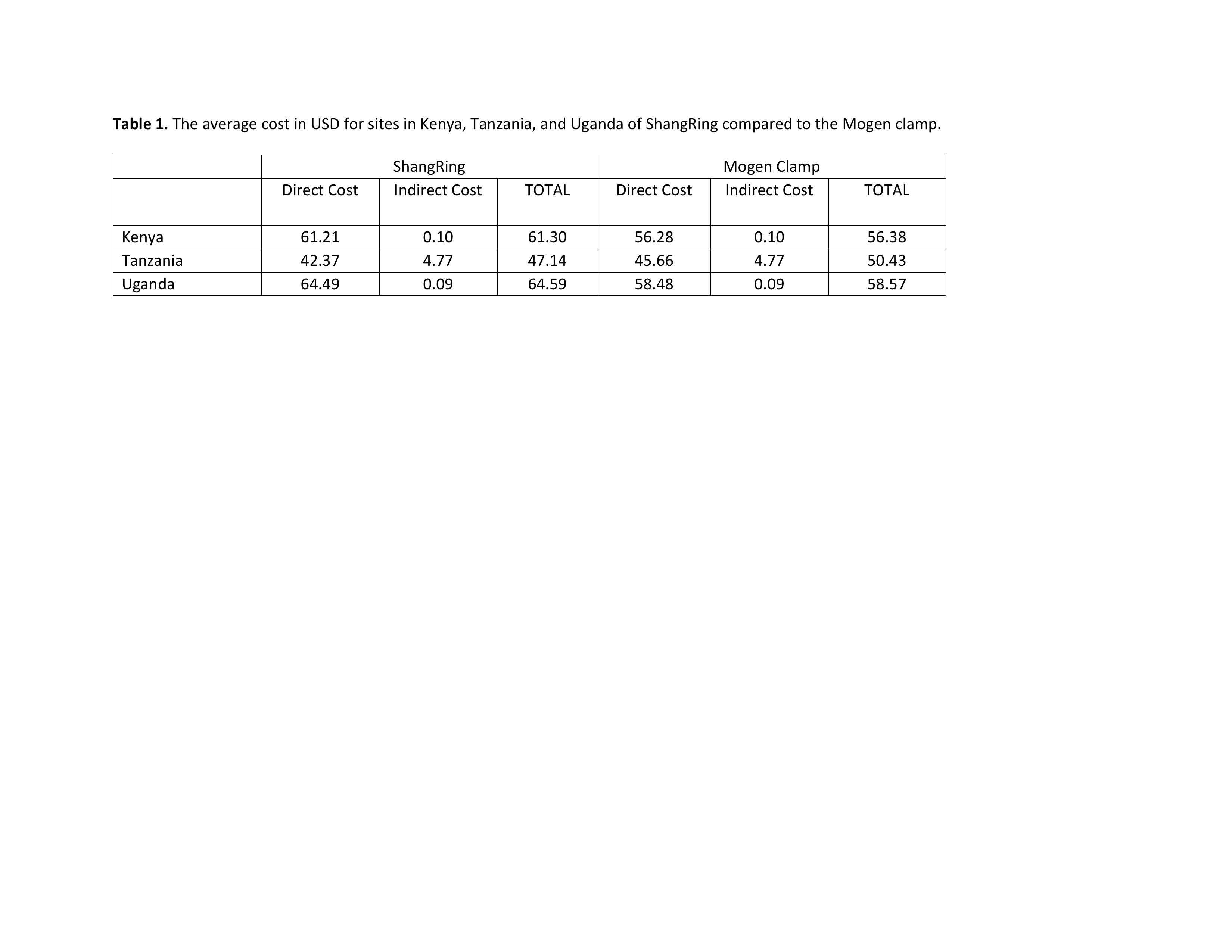
Introduction: The World Health Organization (WHO) has recommended voluntary medical male circumcision (VMMC) as a prevention strategy for countries with low rates of circumcision and high rates of the heterosexually-transmitted human immunodeficiency virus (HIV). Early infant male circumcision (EIMC) is being considered due to its simplicity, rapid wound healing, and similar or more long-term benefits to adolescents and adults. However, data regarding the safety, efficacy, and cost of EIMC are limited. Thus, we sought to perform a comprehensive cost assessment of the ShangRing (SR) versus the standard of care (Mogen Clamp, MoC) as the EIMC device for future scale-up and a cost-effective HIV prevention strategy in this patient population. Methods: As a secondary endpoint to an EIMC randomized controlled trial (RCT) of infants aged 0-60 days in Kenya, Tanzania, and Uganda, receiving SR versus MoC, utilization and cost data were analyzed. This included baseline facility costs, direct costs such as equipment, supply, and personnel costs, as well as indirect costs such as facility maintenance and capital cost for equipment. The Decision Makers Program Planning Tool (DMPPT) v1.0, developed by the USAID Health Policy Initiative in collaboration with UNAIDS, was utilized to perform a direct cost comparison of these two devices. This analysis tool derives a single unit cost of a procedure based on the baseline facility share, direct and indirect costs. All expenses adn costs related to this RCT are are reported in USD. Results: A total of 1378 infant males underwent EIMC, of which 689 had SR, and 689 had MoC. No significant complications required additional cost or intervention at either study site. The overall cost of a single EIMC in Kenya, Uganda, and Tanzania were $61.30, $47.14 and $64.59, respectively for the SR; and $56.38, $50.43, and $58.57, respectively, for the MoC. For both EIMC devices, the costs were mainly driven by direct costs. Conclusions: SR is a safe and low-cost alternative for EIMC in VMMC in Sub-Saharan Africa. Moreover, with scale-up utilizing lower-level personnel, the SR cost may be further reduced. Therefore, the SR is an attractive alternative for future EIMC initiatives in sub-Saharan Africa to further reduce the HIV burden in these regions. SOURCE OF Funding: The Bill and Melinda Gates Foundation