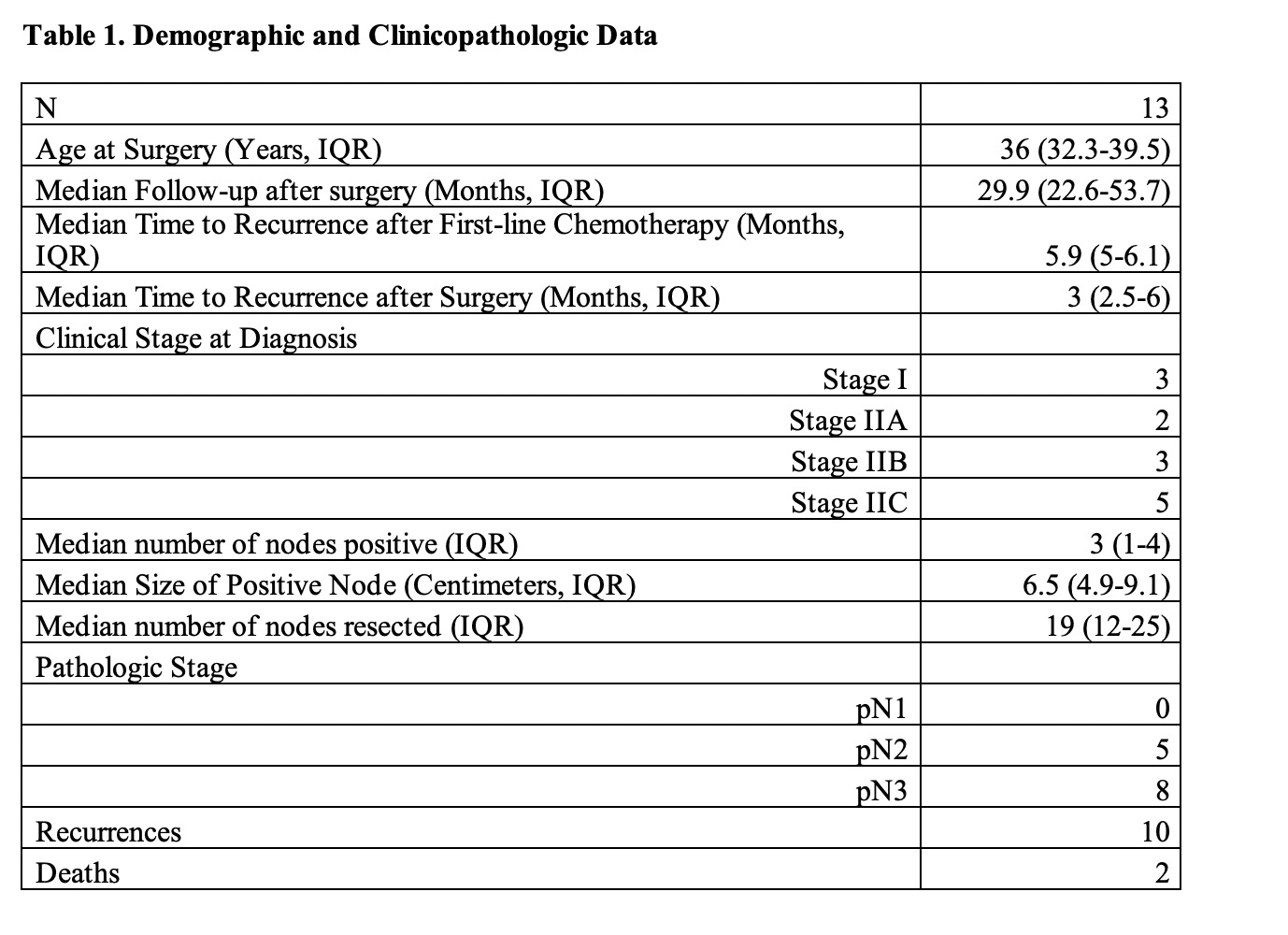
Introduction: Patients with relapsed seminoma after first-line chemotherapy can be treated with salvage chemotherapy or post-chemotherapy retroperitoneal lymph node dissection (PC-RPLND). Based on prior reported experience, surgical management can have worse efficacy and increased morbidity compared to non-seminomatous germ cell tumor. Our aim was to characterize the surgical efficacy and difficulty in a specific cohort of patients with definite progression but minimal disease burden. Methods: The Indiana University testis cancer database was queried to identify men who underwent PC-RPLND for seminoma between January 2011 to December 2021. Included patients only underwent first-line chemotherapy and could not have any evidence of non-seminomatous elements on orchiectomy or have elevated serum alpha-fetoprotein (AFP). All patient demonstrated high suspicion of retroperitoneal disease prior to PC-RPLND was based on increasing size of tumor on standard CT imaging, progression of FDG avidity on PET imaging, or elevated tumor markers. Results: We identified 889 patients that underwent PC-RPLND, of which only 14 patients were operated on for seminoma. One patient was excluded for lack of meaningful follow-up. Out of 13 patients, only 3 patients were disease free with surgery and did not have to undergo salvage chemotherapy. Median follow up time was 29.9 months (IQR: 22.6-53.7). Two patients died due to testicular cancer. The remaining 8 patients were treated successfully with salvage chemotherapy. For additional procedures, 4 patients required a nephrectomy, 1 patient required an aortic graft, 2 patients required a partial ureterectomy, and 3 patients required partial or complete caval resection Conclusions: The decision between salvage chemotherapy and PC-RPLND as second-line therapy can be challenging. Salvage chemotherapy is effective but is associated with short and long-term morbidity. Surgical efficacy in this setting seems to be limited, but careful selection of patients may lead to surgical success without life threatening morbidity or adjunctive procedures that may compromise the ability to receive salvage chemotherapy. SOURCE OF Funding: None