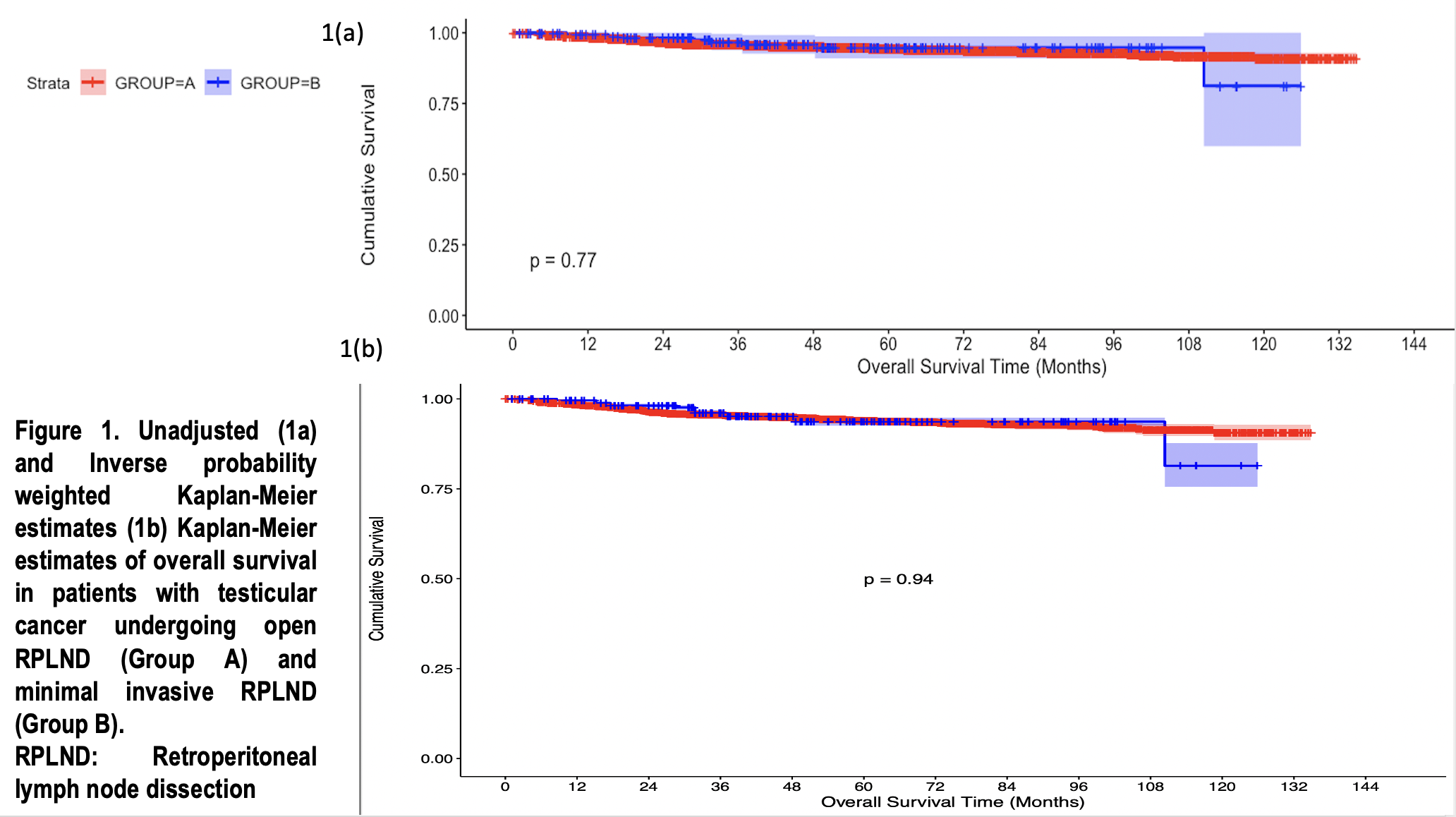
Introduction: Minimal invasive retroperitoneal lymph node dissection (RPLND), either by laparoscopic or robotic approach, has increasingly become popular. However, data comparative data on perioperative outcomes and survival outcomes is limited. In this study, we aim to compare minimal invasive -RPLND (MI-RPLND) with open (O-RPLND) using National Cancer Database. Methods: Using the 2010-2019 National Cancer Database, patients with primary testicular germ cell tumors undergoing RPLND were identified and classified as Group A: O-RPLND and Group B: MI-RPLND. The primary outcome was overall survival (OS). Secondary outcomes included lymph nodal yield, death within 30 and 90 days of surgery, length of stay after surgery, and frequency of unplanned readmission within 30 days of surgical discharge. Inverse probability weighting (IPW) was utilized to balance the two groups. Results: Overall, 3,184 patients were identified; 2971 (93.3%) patients were included in Group A and 213(6.7%) patients were included in Group B. Amongst them, 2419(76%) had NSGCT. Factors associated with increased likelihood of MI-RPLND were treatment at academic research programs (p=0.003) and the treatment period between 2015-2019 (p < 0.001). The median lymph nodal yield in O-RPLND and MI-RPLND group were similar [19 vs 22, p=0.623]. The 5-year OS was similar between the two groups [94.3% in O-RPLND vs 94.7%, in MI-RPLND p=0.77) (Figure 1a). The length of stay after surgery (p=0.623), frequency of unplanned readmission within 30 days of discharge (p=0.728), death within 30-days of surgery (p=0.74) and death within 90-days of surgery (p=0.06) were similar between the two groups. After IPW matched cohort analysis, the 5y-OS remained similar between the open and minimally invasive approach. [93.9% in O-RPLND vs 93.7% in MI-RPLND, p=0.94] (Figure 1b) Conclusions: Both O-RPLND and MI-RPLND are associated with similar OS. In terms of perioperative outcomes, both surgical approaches have similar length of hospital stay, similar rates of mortality within 30-day and 90-day of surgery, and similar rates of unplanned readmission rate within 30 days of surgical discharge. SOURCE OF Funding: None

 photo")