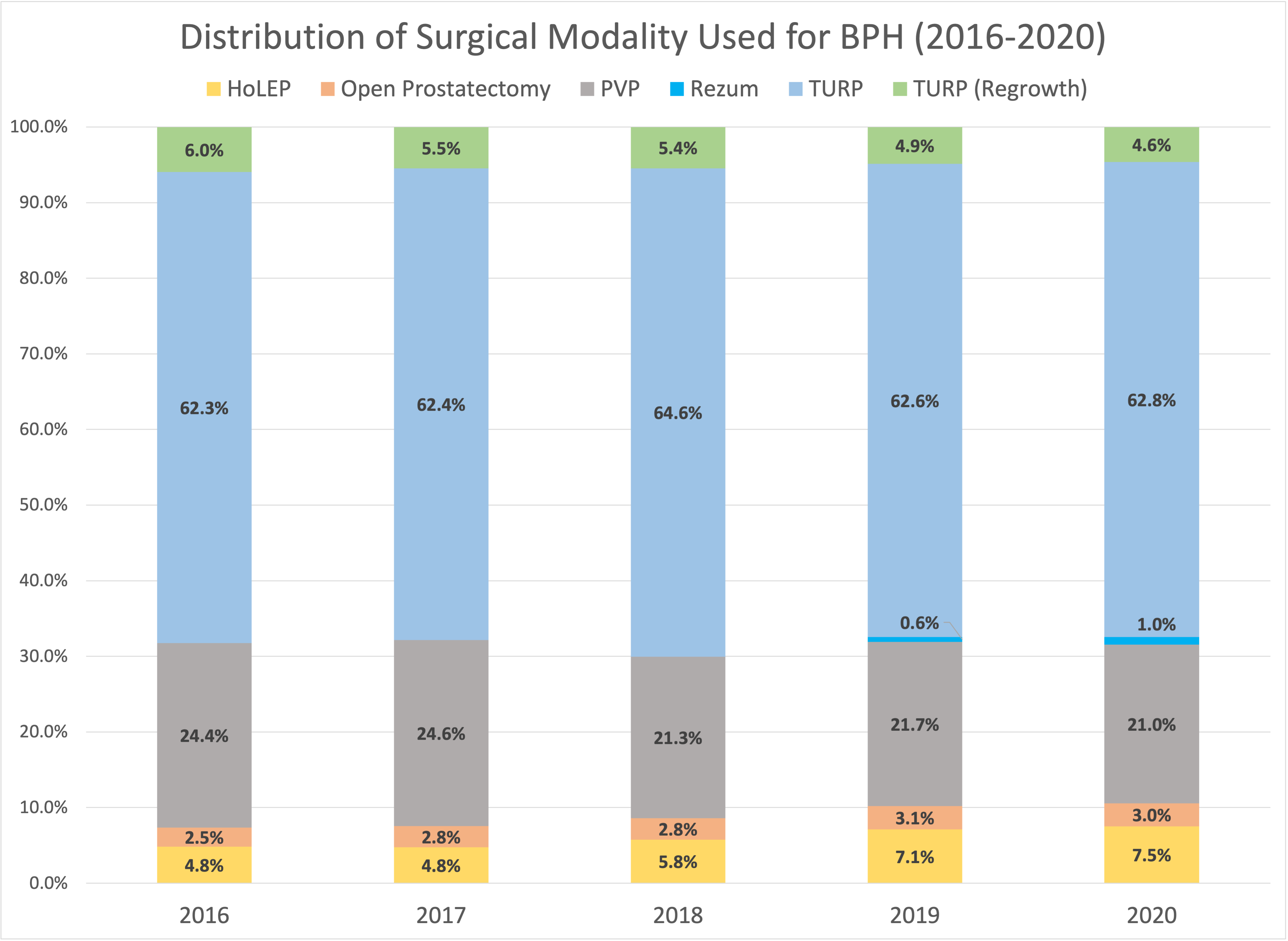
Introduction: The armamentarium for surgical management of benign prostatic hyperplasia (BPH) continues to grow. However, the rates of adoption of multiple techniques over the gold standard have largely been unstudied. Therefore, this study aims to elucidate the most recent trends and safety profile of surgical management for BPH. Methods: Using the American College of Surgeons National Surgical Quality Improvement Program (ACS-NSQIP) database, patients who underwent a BPH procedure from 2016 to 2020 were included (CPT: 52601, 52630, 52648, 55821, 55831, 53854, 52649). Demographic characteristics and the use of each modality were analyzed. The safety profile was assessed by comparing complication rates to transurethral resection of prostate (TURP), which included transfusion rates, urinary tract infection, sepsis, readmission, and death. Chi-square analysis was utilized to determine any significant differences. Results: Overall, 60,291 BPH procedures were performed in the time period studied with an annual average of 12,058. The median age of men undergoing any of the studied modalities ranged from 69-74 years old. White men comprised the largest proportion of the total cohort (63.4%, n = 38,222) followed by Black men (6.4%, n = 3,884). At least two-thirds of all procedures each year were TURP (Figure 1). A significant decline was seen in the use of photovaporization of prostate (PVP) (24.4% in 2016 vs. 21.0% in 2020, p < 0.001). In 2020, 7.5% of all BPH procedures were HoLEP, which is a significant growth from 4.8% in 2016 (p < 0.001). Rezum was introduced in 2019 and accounted for 1% of procedures in 2020. Every procedure studied had limited mortality risk (all <1.0%). Compared to TURP, open prostatectomy had the biggest difference in transfusion rates (12.2% vs. 1.5%, p < 0.001) and readmissions (7.5% vs. 5.6%, p < 0.001), while Rezum has the biggest difference in urinary tract infections (9.7% vs. 5.2%, p = 0.006) and sepsis (2.7% vs. 1.0%, p = 0.02). Conclusions: TURP remains the gold standard for BPH management; however, HoLEP continues to see increased adoption over time. Significant morbidity is seen with open prostatectomy. Infection and sepsis rates from Rezum procedures should be further studied as more patient data becomes available. SOURCE OF Funding: None

 photo")