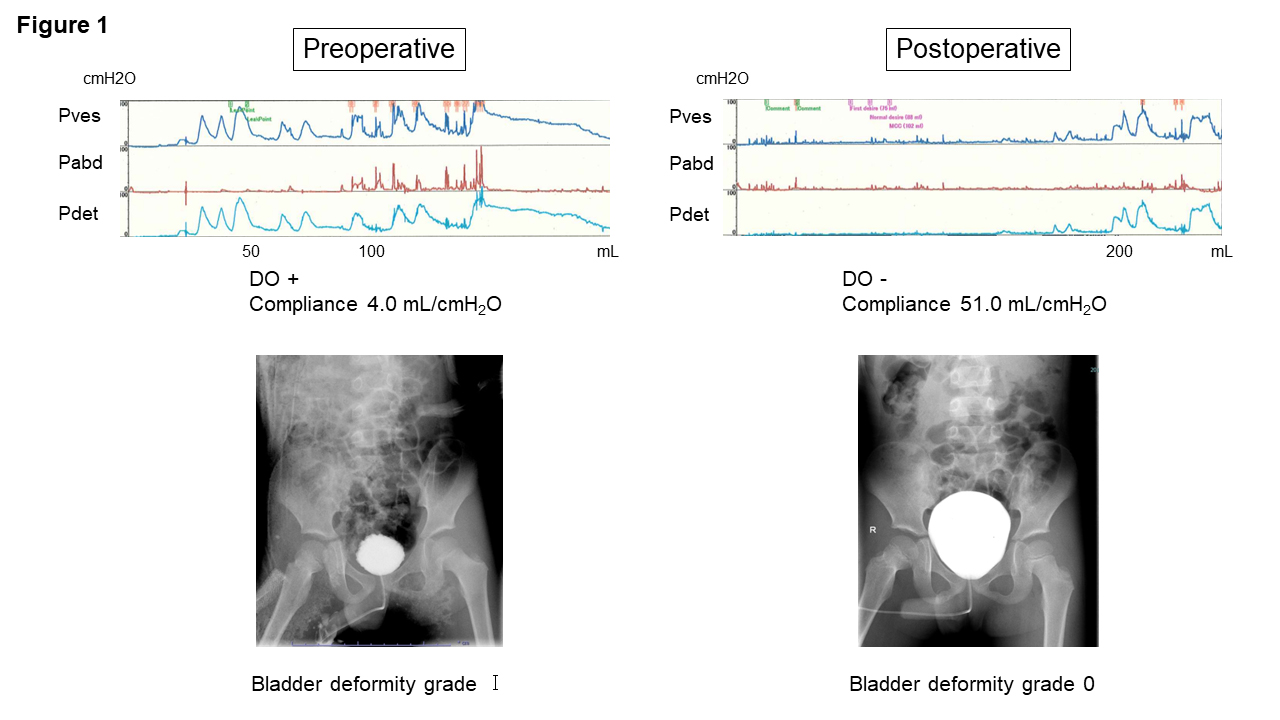
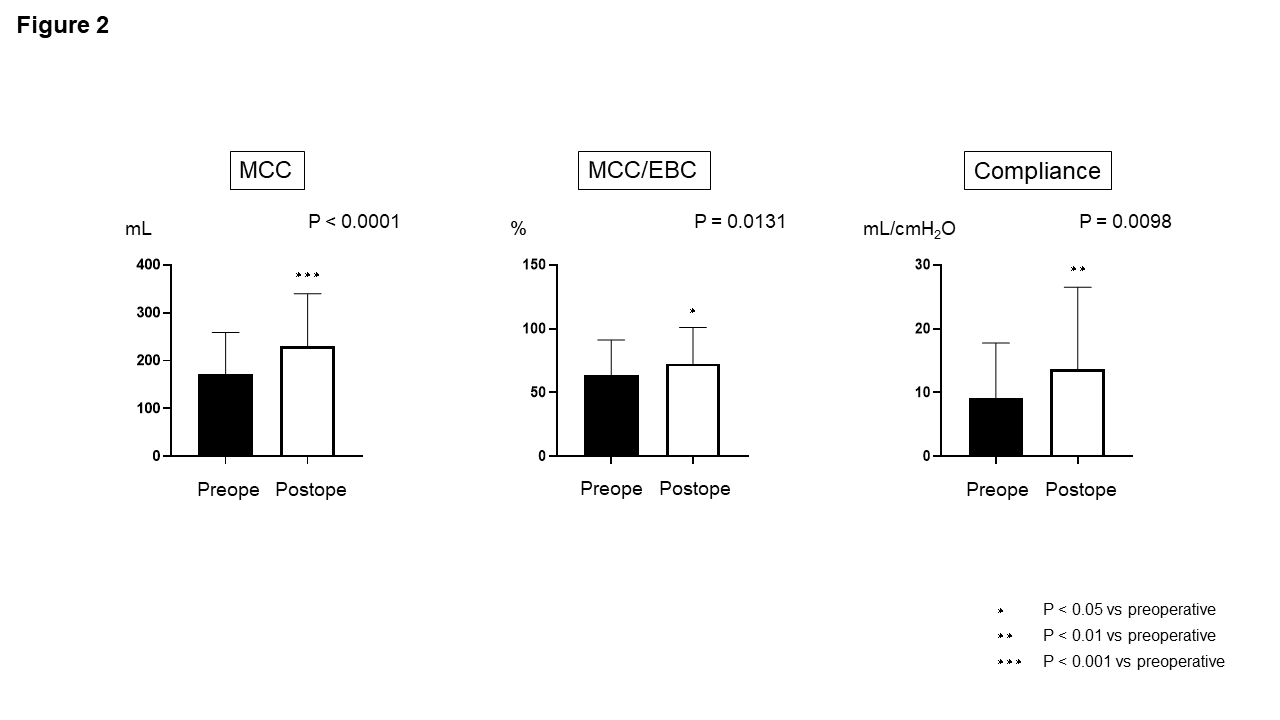
Introduction: Secondary tethering of the spinal cord occurs in 3–30% of patients with history of spinal cord repair of spina bifida. Tethered spinal cord syndrome is characterized by neuropathy that develops when the caudal end of the spinal cord is fixed and gets pulled as the spine grows. These patients show various symptoms of lower urinary tract dysfunction, including urinary incontinence, frequent urination, and dysuria. The main treatment is surgical release of the tethered spinal cord. We evaluated the effect of spinal cord untethering surgery on lower urinary tract dysfunction for secondary tethered spinal cord. Methods: We enrolled patients with spinal cord retethering who underwent untethering surgery at the Department of Urology, Nara Medical University and Hoshigaoka Medical Center between January 1, 2010, and December 31, 2021. We retrospectively evaluated pre- and 6 months postoperative video-urodynamic findings of detrusor overactivity (DO), vesicoureteral reflux (VUR), bladder deformity (BD), maximum cystometric capacity (MCC), MCC/expected bladder capacity (EBC), and bladder compliance. Results: Median age at retethering of the 19 participants included was 9 years. Nine patients had myelomeningocele and 10 had a spinal lipoma. Seventeen patients were managed with self-catheterization. DO was observed in six patients; it disappeared postoperatively in all of them. VUR was observed in three patients, and the severity reduced after surgery in two of them. The Ogawa classification grade of BD improved postoperatively in six patients (Fig. 1). Marked postoperative improvement was also noted in MCC, MCC/EBC, and bladder compliance (pre- vs. postoperative MCC: 172.1 ± 86.7 vs. 231.3 ± 108.9 mL, P < 0.0001; MCC/EBC: 63.8 ± 27.3 vs. 72.7 ± 28.4 %, P = 0.0131; and compliance: 9.1 ± 8.6 vs. 13.7 ± 12.8 mL/cmH2O, P = 0.0098) (Fig. 2). Conclusions: Release of the retethered spinal cord after primary repair improved urine storage function as assessed using video-urodynamics in patients with spina bifida. SOURCE OF Funding: None

 photo")