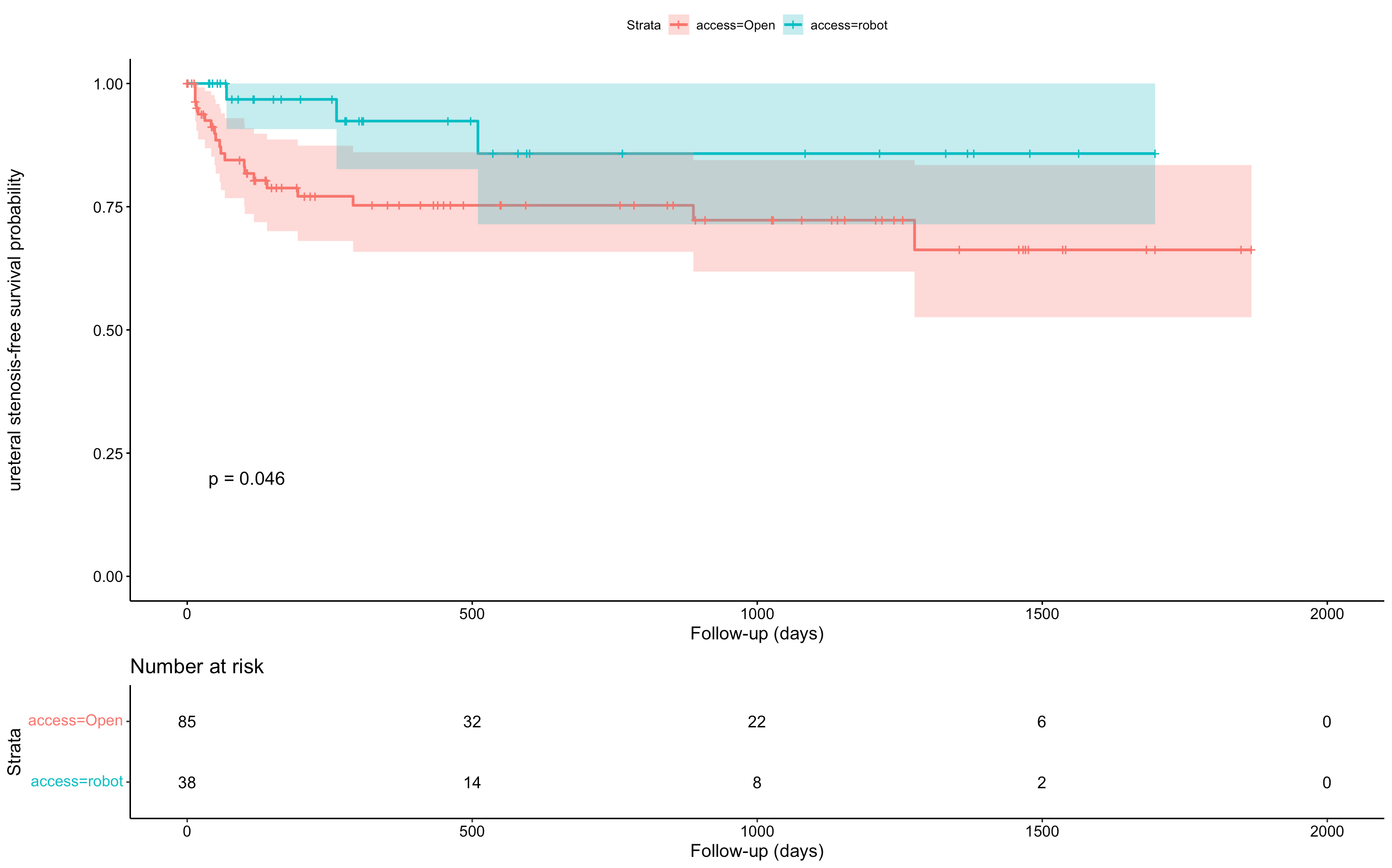
Introduction: Cystectomy associated with non-continent ileal diversion is a common surgery in patients with neurogenic bladder. Few data are available, especially for the robotic approach. Our purpose was to compare open cystectomy (OC) and robot-assisted radical cystectomy (RARC) with ileal conduit, regarding peri- and postoperative outcomes. Methods: We included each patient who underwent cystectomy and ileal conduit for neurogenic bladder in a referral-center between January 2017 and November 2021. Datas were retrospectively analysed. Median follow-up was 16.6 months [IQR: 5; 41]. All patients had neurogenic bladder with failure of conservative treatment and/or impacted Quality of Life (QoL). Open cystectomy with non-continent ileal diversion and robot-assisted cystectomy with intra-corporeal non-continent ileal diversion were compared. Primary endpoint were postoperative complications. Secondary endpoints were length of hospital stay (LOS), surgery duration, blood loss and ureteral anastomosis stricture. Results: A total of 123 patients were included, 85 (69.1%) undergoing OC and 38 (30.9%) RARC. Significant differences were observed for: operative time (OC: 266.9 ± 64 vs. RARC: 205.8 ± 55.5 min, p<0.001), blood loss (OC: 737.7 ± 515.8 vs. RARC: 245.8 ± 169.6 ml, p<0.001), delay until feeding resumption (OC: 7.1 ± 4.7 vs. RARC: 5.5 ± 2.9 days, p=0.05) and mean LOS (OC: 21.6 ± 13.9 vs. RARC: 16.2 ± 7.6 days, p=0.03). In RARC group, there were 10.5% complications Clavien-Dindo >2 whereas 23.8% complications underwent in the OC group (p=0.1). With regards to uretero-ileal anastomosis stenosis, 23 (18.7%) events occurred after a median follow-up of 16.6 months [IQR: 5; 41] including 20 (23.5%) and three (7.9%) in the ORC and RARC groups, respectively (p=0.07). Patients who underwent RARC had better ureteral stenosis-free survival rates than those who underwent ORC (log-rank test, p=0.05). Conclusions: RARC is a safe approach for management of neurological bladder showing significantly better perioperative outcomes. SOURCE OF Funding: None

.jpg "Jeanne Beirnaert (she/her/hers) photo")