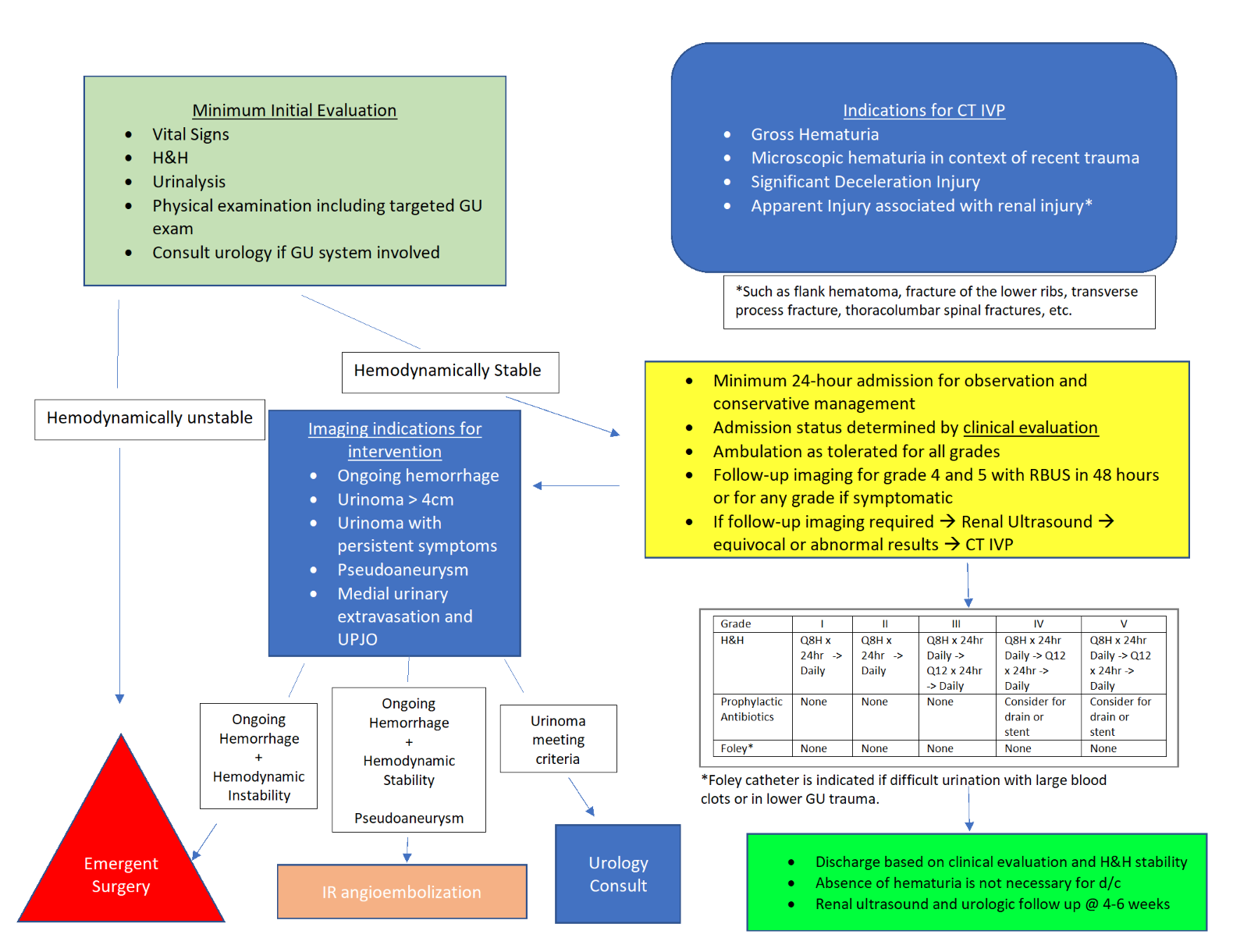
Introduction: There is no consensus on the ideal management of pediatric renal trauma (PRT); therefore protocols tend to be institution-specific. This study aimed to characterize PRT at a rural level-1 trauma center and to develop a standardized protocol. Methods: We retrospectively reviewed a prospectively maintained database of PRT at our institution from 2009-2019. Injuries were characterized based on renal trauma grade, associated multi-organ involvement and need for intervention. We subsequently appraised the benefit of patient transfer from regional hospitals and the impact of follow-up imaging on patient care. Results: Of the 250 patients admitted with a diagnosis of renal trauma, 50 were under the age of eighteen. Of those, 32/50 (68%) patients had low-grade (grade I-III) injuries with the remaining 18/50 (32%) diagnosed with high grade (IV-V) injuries. All grade I-III injuries were managed conservatively without requiring invasive intervention. Among patients with low-grade trauma, 21/32 (65.5%) were transferred from an outside facility. For patients with high grade injuries, 9/18 (50%) required surgical intervention. Of the patient with high grade injuries, 2/18 (11%) had their management escalated as a result of follow up imaging. Based on data from our institution, we developed pediatric-specific renal trauma protocol which was implemented in early 2021 (Figure 1). Conclusions: Isolated, low-grade PRT can be managed conservatively at regional hospitals without needing transfer to a Level 1 Trauma Center. However, those with high-grade injuries should be monitored closely as these patients may require intervention. Development of PRT protocol will help to safely triage this population and identify those that require transfer to tertiary care center. SOURCE OF Funding: None