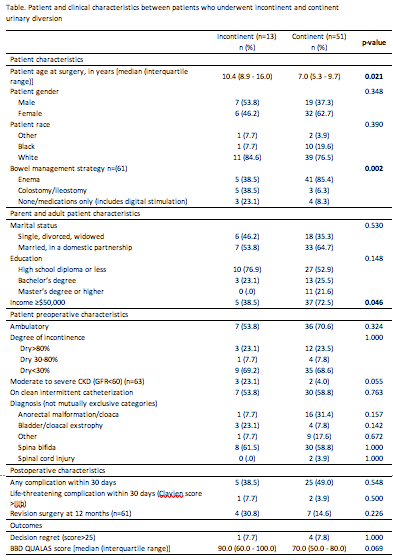
Introduction: Continent or incontinent urinary tract reconstruction may be needed in pediatric patients with neurogenic bladder (NGB) to achieve continence per urethra. Choosing a reconstructive technique involves shared decision-making. We aimed to compare decisional regret (DR) and quality of life (QOL) in NGB patients who underwent continent vs. incontinent reconstruction, hypothesizing there would be no difference in DR and QOL between groups. Methods: This was a single-institution retrospective cohort study. We included NGB patients who underwent urinary tract reconstruction from 2010-2020. The continent group included those who underwent bladder augmentation or neobladder, and the incontinent group was those who underwent a chimney or conduit procedure. We excluded patients <4 years of age, with severe developmental delay, or unable to speak English, and those with follow-up <1 year. The patient/legal guardian completed a demographic questionnaire and validated Decisional Regret Scale (DRS). The patient completed the QUALAS, a measure of QOL applicable to NGB. Other clinical information was collected via chart review. Our primary outcome was measured by DRS score, in categorical fashion (0-25=no/mild regret, >25=moderate/severe regret). Our secondary outcome was measured by the continuous score (max score 100) on the bladder/bowel domain (BBD) of the QUALAS. Chi square / Fisher exact test, t-tests, or Mann Whitney tests were used to assess differences between groups. Results: 95 patients (70 continent) met inclusion criteria. Survey response rate was 67% (51 continent, 13 incontinent). Patients in the incontinent group were older at time of surgery. More patients in the continent group had a household income of =$50,000. There was a higher frequency of enema use for bowel management in the continent group. There were no differences between groups in frequency of patients with moderate/severe DR and in median BBD QUALAS score. Conclusions: We found no differences in DR and QOL in patients who underwent continent vs. incontinent reconstruction. Patients who are older at time of continence readiness, from families with lower household income, and unable to perform enemas may be more likely to benefit from incontinent reconstruction. SOURCE OF Funding: NURAG Grant Nationwide Children's Hospital