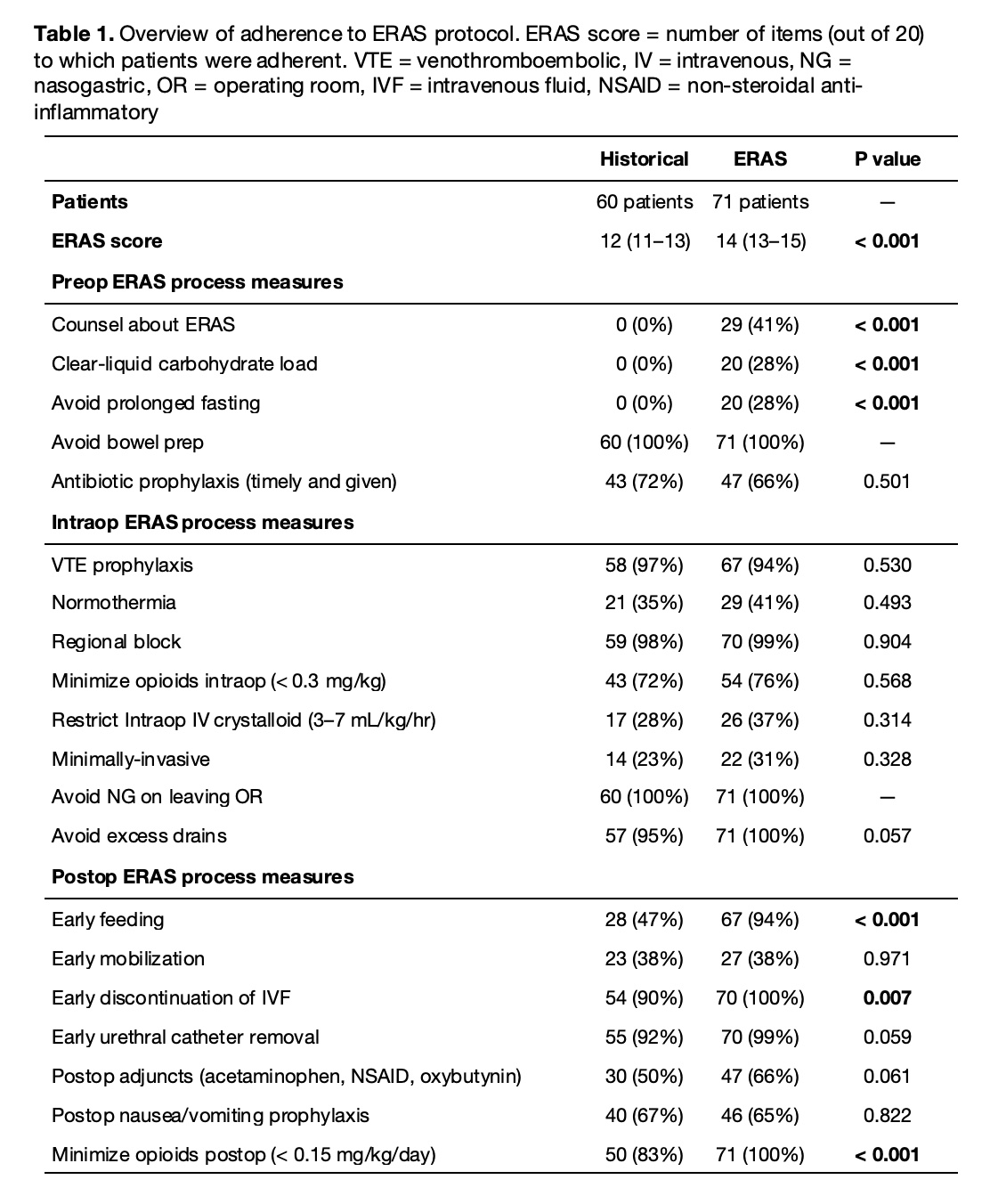
Introduction: Enhanced Recovery After Surgery (ERAS) is a set of perioperative strategies to improve surgical recovery. Though it has gained traction in adults, it has been less studied in pediatrics. A standardized ERAS protocol for complex lower urinary tract reconstructive surgeries was introduced in 2014 at our institution. ERAS was expanded to all urologic surgeries requiring an inpatient admission (e.g., extended recovery) in 2018. We hypothesized that patients receiving care under ERAS would have fewer complications than recent historical controls Methods: In fall 2018, stakeholder consensus was sought to create an ERAS protocol for ureteral operations, pyeloplasty, non-oncologic nephrectomy, and urachal excisions. Input from urology, anesthesia, and nursing was sought. Patients from a single center were retrospectively reviewed from an IRB-approved database including patients who received ERAS protocol (2018–2022) and recent historical controls (2016–2018). Twenty ERAS measures were included in the protocol and tracked for each patient. Outcomes were 30-day complications, protocol adherence, length of stay (LOS), opioid requirements, and unexpected healthcare encounters (ED visits, re-admissions, reoperations) within 30 days. Results: 131 patients were included (60 historical and 71 ERAS). Patients were demographically similar, though the historical group had a higher percentage of comorbidities (6.7% of controls had kidney transplant history vs 0% in ERAS, p<0.05). Adherence to protocol measures was improved in the ERAS group (14 [13–15] vs 12 [11–13], p<0.001). Individual process measure compliance is illustrated in Table 1. LOS, maximum PACU pain scores, and opioid prescriptions decreased in the ERAS group (1.2 days [1.1–1.3] vs 1.3 days [1.2–2.2], p<0.001; 4 [0–6] vs 0 [0–3], p<0.05; and 39% vs 80%, p<0.001, respectively). There was no difference in unscheduled healthcare encounters, though the ERAS group did have a lower 30-day complication rate (0.2 vs 0.5 complications per patient, p<0.006). Most complications for both groups were Clavien-Dindo grade 1. Conclusions: ERAS improves outcomes across multiple measures in pediatric patients undergoing common urologic surgeries that typically involve in a short-stay admission. These findings should be corroborated on a larger scale. SOURCE OF Funding: None