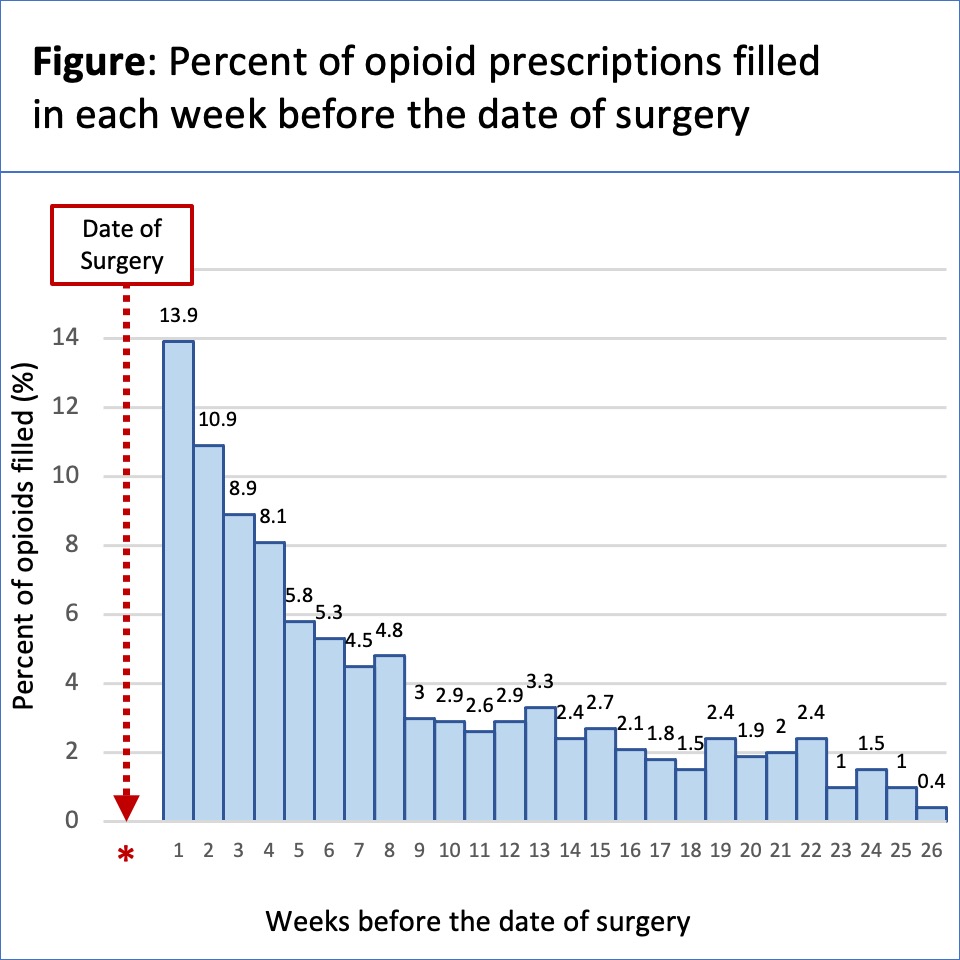
Introduction: Most post-operative opioid prescribing guidelines are restricted to opioid naïve populations due to a dearth of data regarding pre-operative opioid use. We aim to quantify pre- and post-operative opioid prescribing patterns among patients undergoing a major cancer surgery and measure the association between pre-operative opioid exposure and post-operative prescribing. Methods: We used the Wisconsin Health Information Organization database, which includes commercial-payer, Medicare Advantage and Medicaid claims and captures over 75% of Wisconsin’s population. We collected demographic data on adult patients undergoing radical prostatectomy and partial or radical nephrectomy between 1/1/2017 and 12/31/2021. We evaluated pre- and post-operative opioid prescriptions, quantified opioid exposure in morphine milligram equivalents (MME), and compared prescribing characteristics between opioid naïve and opioid exposed patients (defined as those with a filled prescription in 6 months before surgery). Results: We identified 3,693 patients (2,306 prostatectomy; 1,387 partial or radical nephrectomy). 23% of patients were exposed to opioids prior to surgery (18% prostatectomy, 30% nephrectomy). The median pre-operative dose was 202 MME (IQR 100-600), and fills occurred at a median time of 42 days (IQR 18-91), with increasing frequency in the weeks prior to surgery (Figure). After surgery, 55% of patients filled an initial opioid prescription, with a median first dose of 171 MME (IQR 100-334), equivalent to 23 oxycodone 5mg tablets. Opioid exposed patients had a significantly higher two-week post-operative dose (238 vs 142 MME, p<0.001) and number of prescriptions filled (1.46 vs 1.23, p<0.001). Conclusions: Nearly one quarter of prostatectomy and partial or radical nephrectomy patients are exposed to opioids prior to surgery. Post-operative prescribing remains at levels twice the guideline recommendations for all patients, even higher in patients with prior exposure. Understanding the implications of prior opioid exposure on the management of postoperative pain and opioid use is imperative to inform real-world care and guideline recommendations. SOURCE OF Funding: AHRQ K08HS028474 award

 photo")