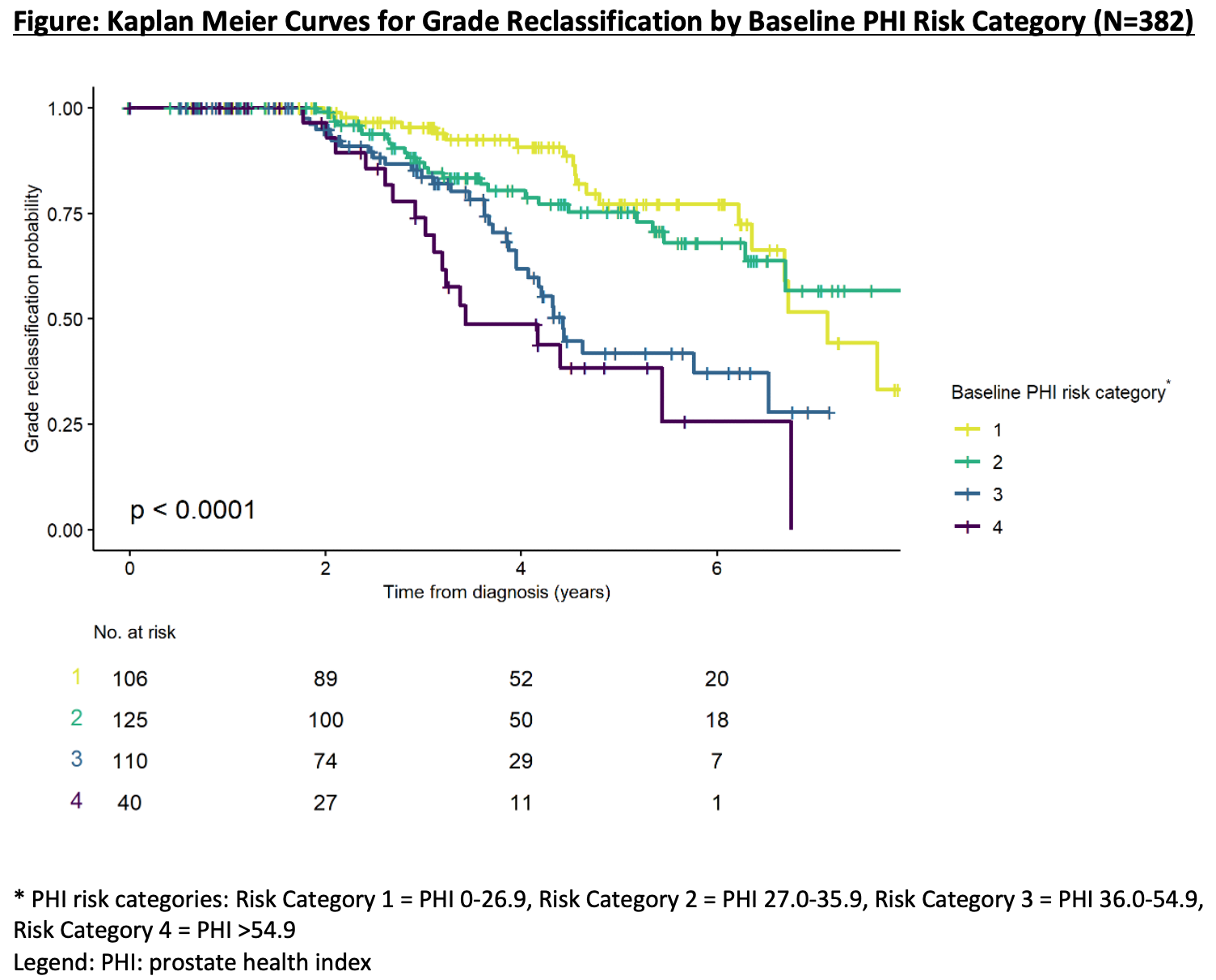
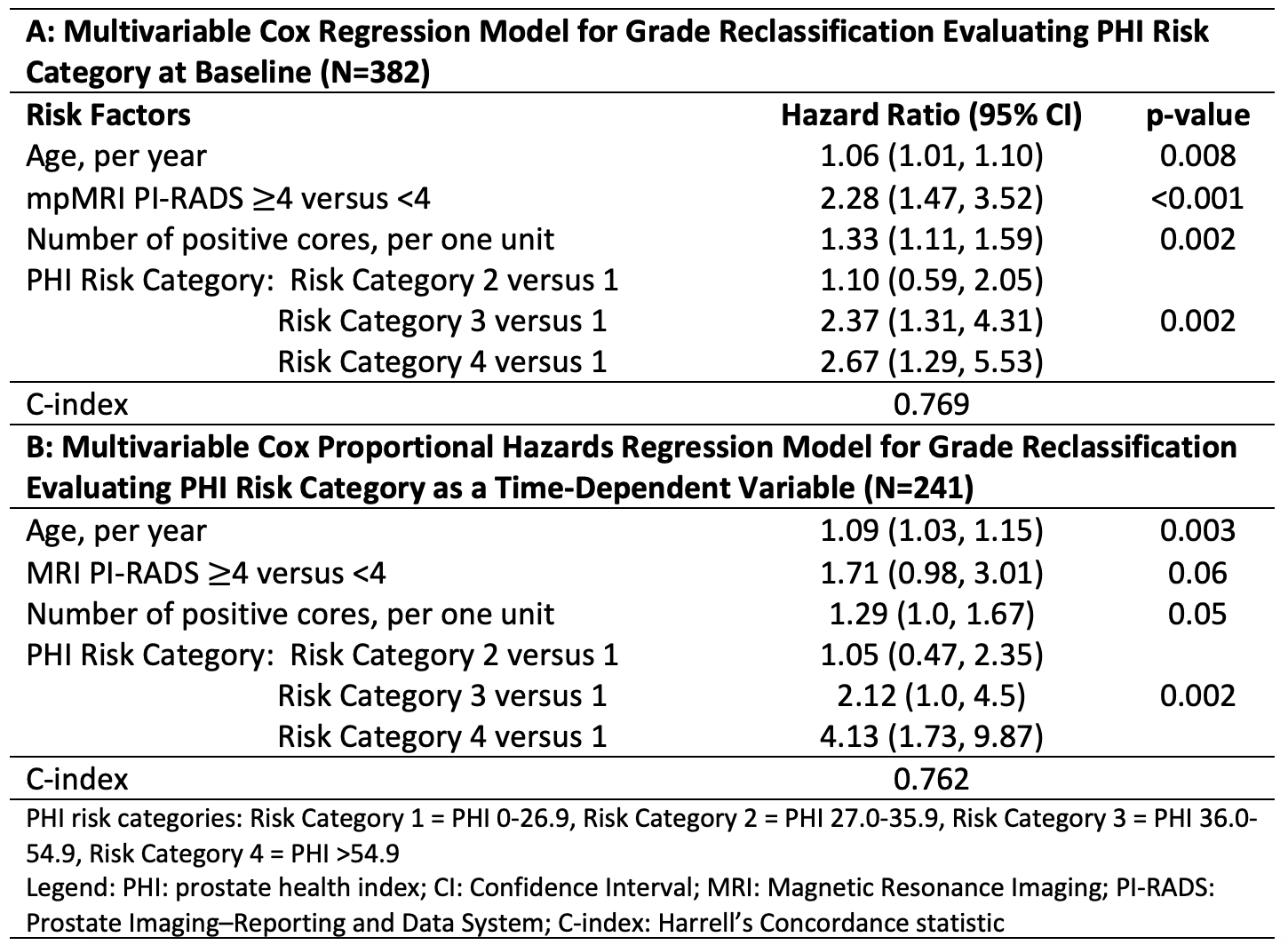
Introduction: We sought to determine if repeated prostate health index (PHI) tests during active surveillance (AS) are of clinical value in a contemporary AS cohort followed with multiparametric magnetic resonance imaging (mpMRI) and biopsies of the prostate. Methods: We identified 382 patients in our AS program with at least one mpMRI and one PHI test, of which 241 had at least two PHI tests. All men had =Grade group 1 (GG1) prostate cancer on diagnostic and confirmatory biopsy. Grade reclassification (GR) was defined as =GG2 identified on surveillance biopsy. PHI risk categories 1-4 were as defined by the manufacturer. A multivariable Cox proportional hazard regression model was performed to evaluate the association between baseline PHI risk category and GR, and change in PHI risk categories over time and GR, respectively. Results: Men with baseline PHI scores in the highest risk categories had lower rates of GR-free survival (log-rank p<0.001; Figure). On multivariable Cox regression baseline PHI risk category was a predictor of GR (model C-index 0.769; Table A). Men with an increase in PHI risk category or consistently high PHI (risk category 3-4) (compared to baseline PHI) experienced more upgrading (36/112=32.1% vs 27/129=20.9%, p=0.048). On multivariable Cox proportional hazards model with PHI risk category as a time-dependent variable, increasing PHI risk category demonstrated increasing association with GR (model C-index 0.762, Table B). Conclusions: Both baseline PHI risk category and PHI risk category over time were predictors of GR after confirmatory biopsy. The model with PHI category changes over time did not perform better than the model with baseline PHI risk category. PHI is a non-invasive and easy to obtain test, so further evaluation of its clinical utility in reducing the frequency of mpMRI and/or surveillance biopsies and in improving risk stratification is warranted. SOURCE OF Funding: Ralph T. and Esther L. Warburton Foundation and Dr. Hugh Judge Jewett Fellowship in Urologic Oncology.