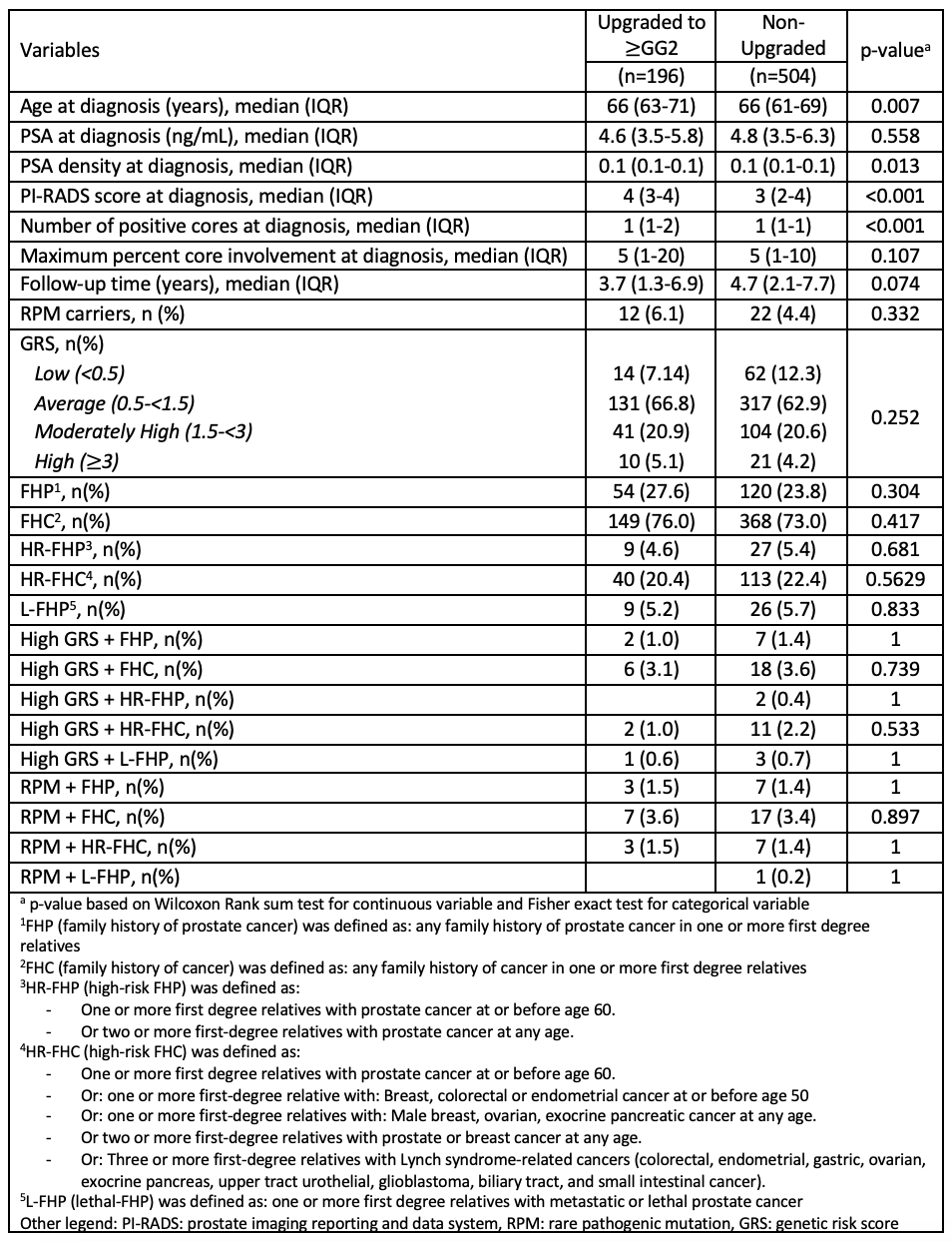
Introduction: In this study, we sought to evaluate the impact of three measures of inherited risk (rare pathogenic mutation (RPM) carrier status, single nucleotide polymorphism (SNP) -based genetic risk score (GRS) and various definitions of family history (FH)) on upgrading during active surveillance (AS). Methods: We identified 700 men enrolled in the Johns Hopkins AS registry from 1995 to 2018 with available sequencing data. All men had GG1 disease at diagnosis. A multivariable proportional hazards model was used to assess the association between RPM carrier status, GRS and FH and upgrading defined as the detection of Grade group (GG) =2 PCa on a surveillance biopsy, adjusting for age, PSA density, cancer volume metrics, and Eigen values (genetic background). RPM carrier status was defined as being a carrier of any one of the following gene mutations: BRCA1, BRCA2, ATM, PALB2, CHEK2, MLH1, MSH2, MSH6, PMS2, or HOXB13. GRS was defined as: low ( <0.5), average (0.5 – 1.5), moderately high (1.5 – 3), and high (=3). Various definitions of FH were used: any FH of PCa (FHP), any FH of cancer (FHC), high-risk FH of PCa (HR-FHP) and high-risk FH for any cancer (HR-FHC) based on National Comprehensive Cancer Network guidelines, and history of lethal PCa (L-FHP). Results: Among the 700 AS patients, 34 were RPM carriers (4.9%), 31 had a high GRS (4.4%), 174 (24.9%) had a FHP, 36 (5.1%) had a HR-FHP, 517 (73.9%) had a FHC, 153 (21.9%) had a HR-FHC, and 35 (5.0%) had a L-FHP. Overall, 196 (28.0%) patients upgraded on surveillance. There was no significant difference in RPM status, GRS, or FH (using any of the FH definitions) between men who upgraded and men who did not (Table). In addition, men with high GRS and positive FH, and RPM carriers with a positive FH, did not experience more upgrading, regardless of the definition used for FH (Table). On multivariable analysis neither RPM carrier status, GRS or FH (using any of the FH definitions) nor any of the three measures of inherited risk combined were predictors of upgrading (p>0.05). Conclusions: In a large cohort of AS men with GG1 PCa, neither RPM carrier status, high GRS, positive FH nor combinations of the three predicted upgrading on AS, suggesting that such men can be safely monitored on AS. This study is limited by low number of RPM carriers and low number of men with high GRS. SOURCE OF Funding: Ralph T. and Esther L. Warburton Foundation and Dr. Hugh Judge Jewett Fellowship in Urologic Oncology.