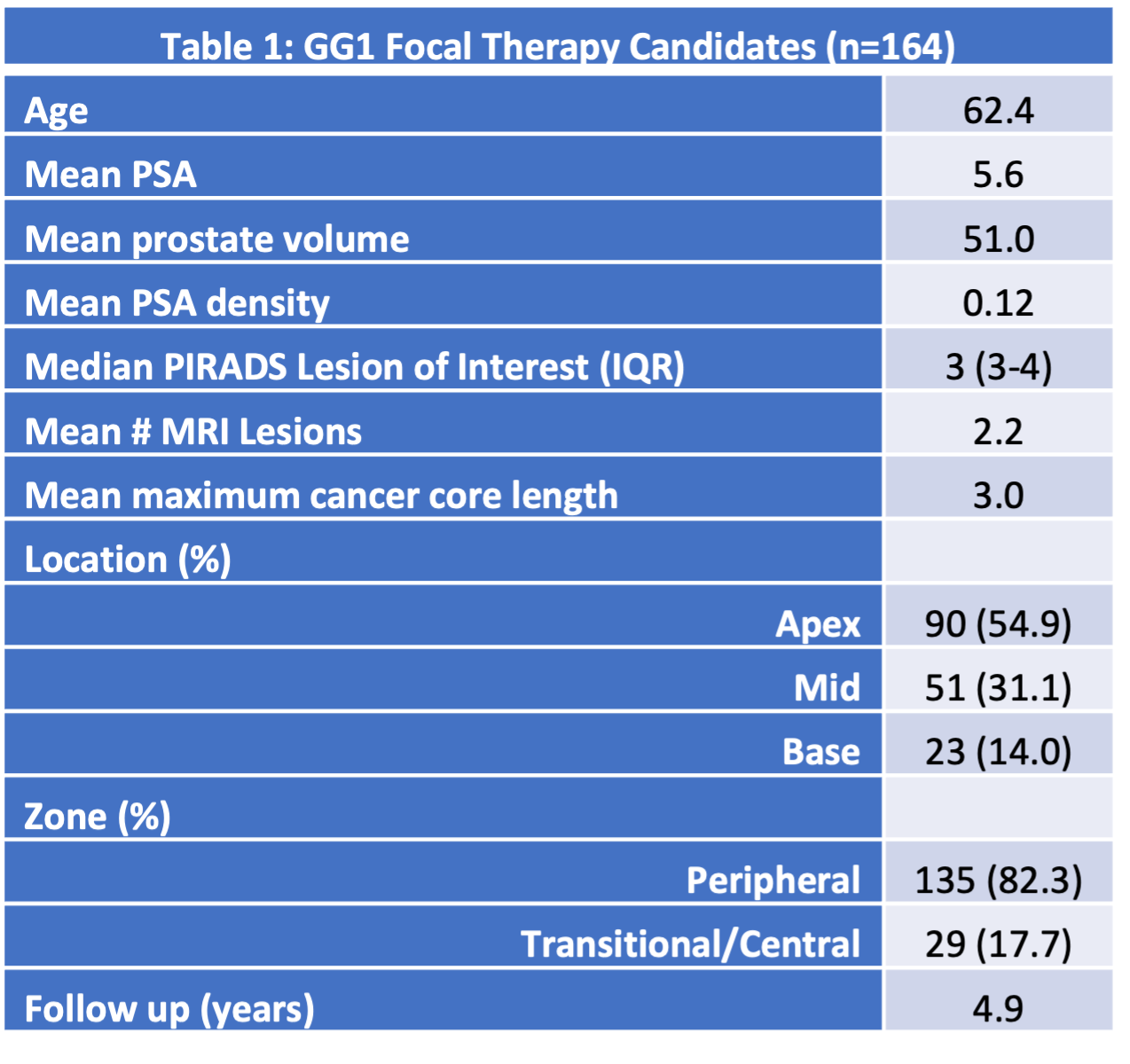
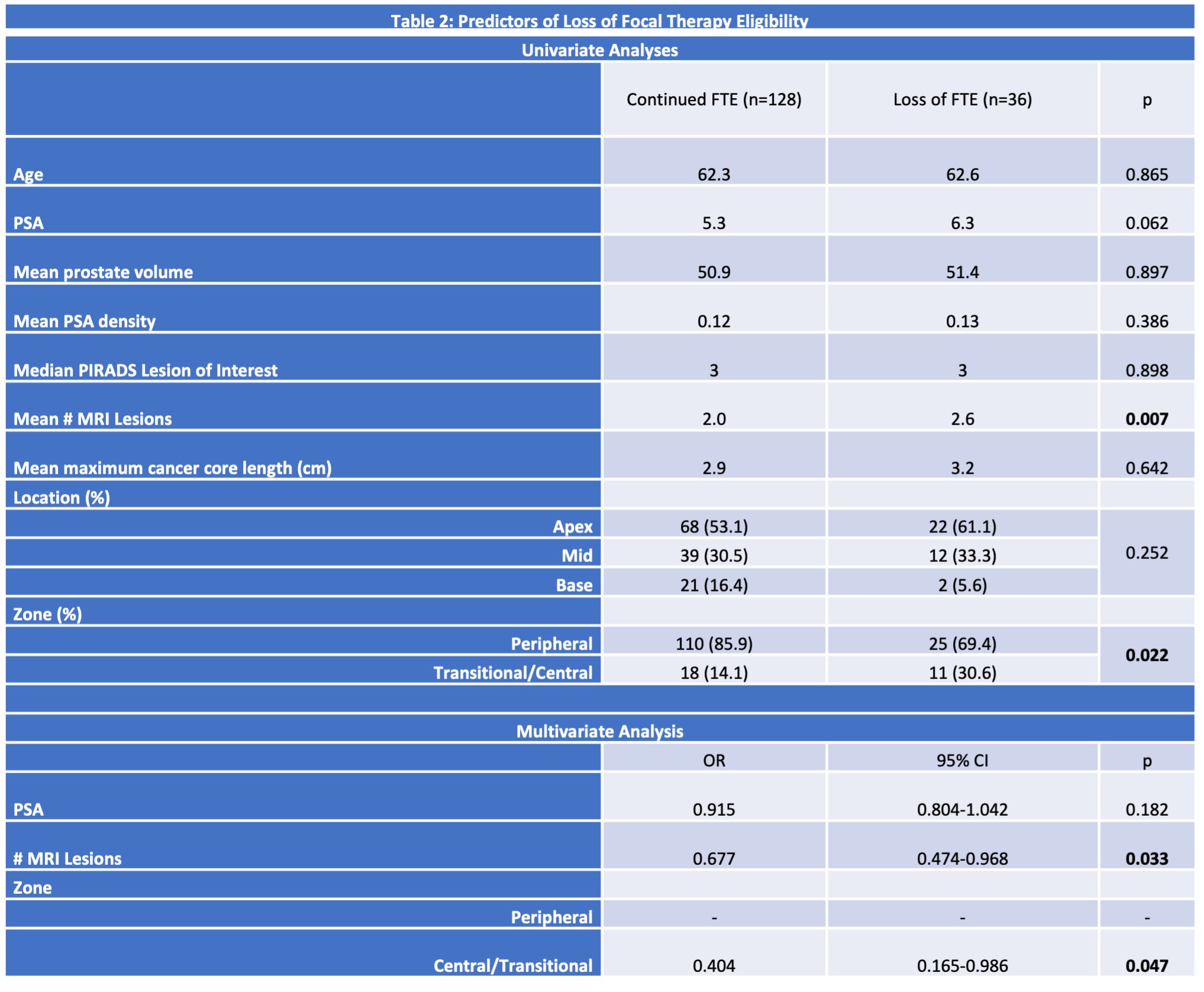
Introduction: Focal Therapy (FT) for Gleason grade group (GG) 1 prostate cancer (PCa) is controversial, given almost all of these patients are suitable active surveillance (AS) candidates. Little is known about how many AS GG 1 patients retain focal therapy eligibility (FTE) over time. The objective of this study is to evaluate initial and long-term FTE for patients with GG1 disease. Methods: A prospectively maintained AS cohort was retrospectively queried for patients initiated on AS between 2009 and 2020 with GG1 PCa. Patients with a unilateral, biopsy-concordant, MRI-visible PIRADS or PIRADS-equivalent 2-5 lesions amenable to hemiablation who had a PSA <20, <4 positive systematic biopsy cores were considered FTE. Patients who remained GG1 were considered to have maintained FTE. Those who progressed were reassessed at time of progression for FTE. Patients with =GG4 disease, bilateral GG=2, or MRI-invisible GG=2 lost FTE. Univariate and multivariate analyses were conducted to evaluate factors associated with FTE. Results: 282 GG1 PCa patients were identified, 164 of whom (58%) were FT candidates, with a mean follow-up of 4.9 years (range 1.0-13.4 years). 81/164 (49%) progressed to GG=2 or higher on a subsequent biopsy. At the time of PCa upgrading, 36/164 (22%) of the FT candidate cohort lost FTE. Baseline characteristics are shown in Table 1. Patients who lost FTE trended toward increased PSA (6.3 vs 5.3, p=0.062 and MRI lesions (2.6 vs 2.0, p=0.007), and were more likely to have transitional or central zone (TZ/CZ) lesions (30.6% vs 14.1%, p=0.022) relative to those who maintained FTE. On logistic regression (Table 2), the number of MRI lesions and TZ/CZ lesions were associated with FTE loss (p=0.033 and 0.047, respectively). Conclusions: While approximately half of GG1 FT candidates demonstrate disease progression, almost 80% maintain FTE. Given the demonstrated safety of AS and relatively small number of patients who lose FTE while on surveillance, routine FT for GG1 disease would result in a large number of unnecessary procedures. SOURCE OF Funding: none