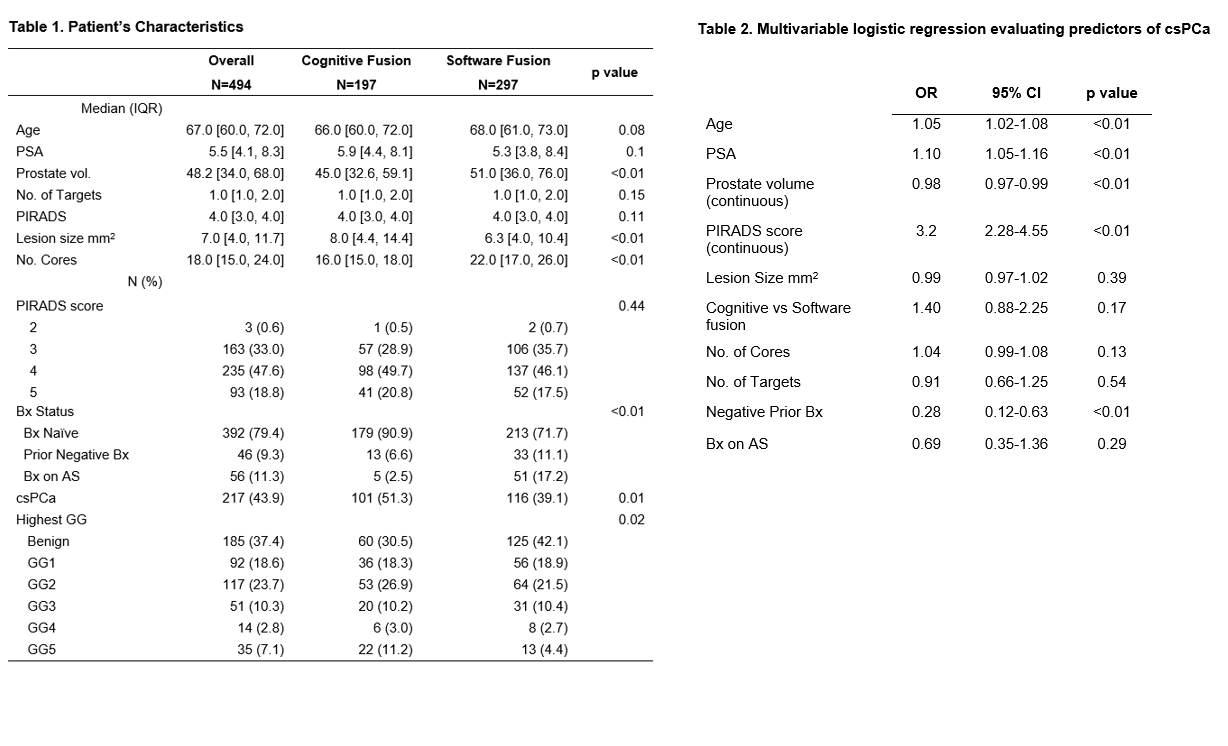
Introduction: Transrectal ultrasound guided biopsy (TR-Bx) is the predominant method of prostate cancer diagnosis in the US with transperineal prostate biopsy (TP-Bx) gaining adoption owing to a lower risk of infection. Landmark studies have demonstrated that MRI prior to TR-Bx improves detection of clinically significant prostate cancers (csPCa), and several software fusion platforms exist to aid in needle targeting. The use of cognitive or software fusion in the TP-Bx setting has not been explored. We sought to evaluate the detection rate of csPCa in TP-Bx performed with MRI targeted cognitive fusion (CF) versus software fusion (SF). Methods: A multicenter retrospective cohort of men undergoing MRI guided TP-Bx for the indication of elevated PSA, suspicious lesion on MRI, or active surveillance, were included in this study. Variables included age, PSA, prostate volume, PIRADS scores, number of cores sampled, and pathologic outcomes. CF and SF techniques were selected based on surgeon preference, utilizing either the PrecisionPoint system (Perineologic, Cumberland, MD) or standard stepper and brachytherapy grid. Systematic biopsies along with MRI targeted cores were obtained for all patients. Multivariable logistic regression was used to determine factors associated with csPCa. Results: In total, 494 men (197 cognitive, 297 software fusion) underwent MRI guided TP-Bx. Baseline age, PSA, number of targets, and PIRADS scores were similar among both groups (Table 1). A higher proportion of men who underwent CF were biopsy naïve (90% vs 72%, p= <0.01). Significantly more cores were obtained in the SF group (median 22 (17 – 26) vs 16 (15 – 18), p < 0.01) and target sizes were smaller in the SF group, median 6.3 mm2 (4 mm2-10.4 mm2) vs 8 mm2 (4.4 mm2-14.4 mm2), p < 0.01). The unadjusted detection rate of csPCa was higher in the CF group (51% vs 39%). On multivariable analysis fusion technique was not a predictor of csPCa glandwide (OR 1.4, 95% CI 0.88 – 2.25, p=0.17), or in the target lesion specifically (OR 0.98, 95% CI 0.57-1.68, p=0.95). Conclusions: Our multicenter analysis demonstrates no difference in the detection of csPCa in TP-Bx utilizing MRI guided CF vs SF. Since SF platforms are quite costly, CF via TP-Bx is appealing as it is not only safer than TR-Bx but also more cost-effective than using SF technology. SOURCE OF Funding: None

 photo")