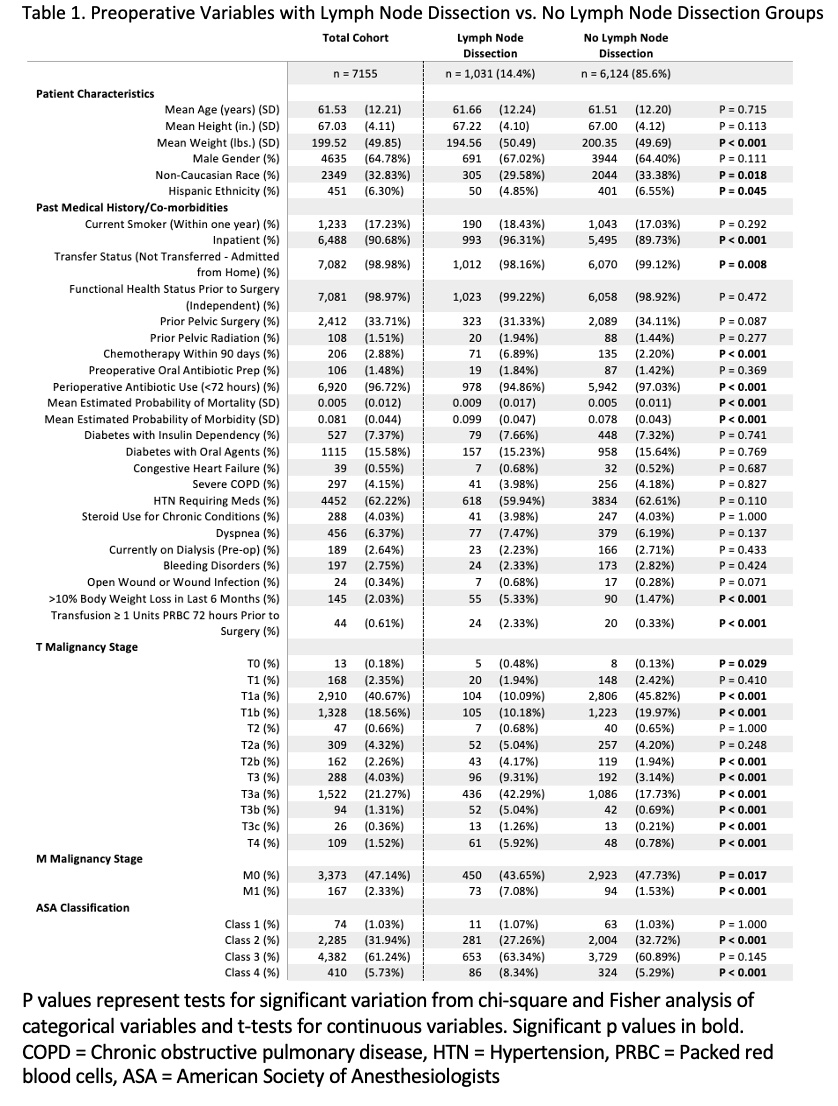
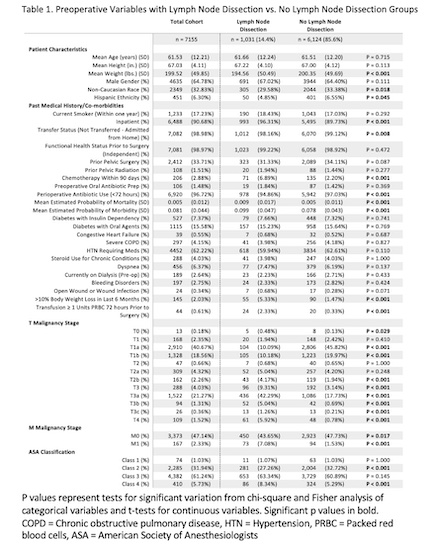
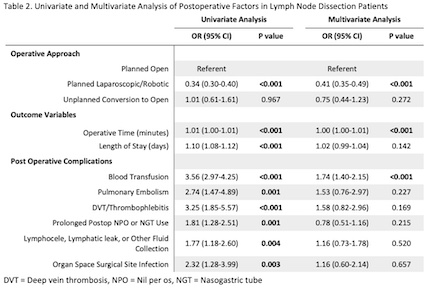
Introduction: Renal cell carcinoma (RCC) accounts for 2-3% of all cancers. Although RCC does not follow the typical lymphatic spread pattern seen in other urologic malignancies, lymph node dissection (LND) may be performed in conjunction with nephrectomy to assist in staging. The objective of this analysis is to compare the frequency of postoperative complications among patients undergoing nephrectomy with or without LND. Methods: The 2019 & 2020 American College of Surgeons National Surgical Quality Improvement Program (ACS NSQIP) database was analyzed for patients who underwent partial or radical nephrectomy for kidney cancer. The groups were then subcategorized into LND and no LND. Fisher’s exact tests for continuous variables and Chi-squared analysis for categorical variables were performed. Multivariable logistic regression was performed for the statistically significant variables on the T-test/Welch-test and Chi-squared analysis between the LND and no LND groups. Statistical significance was accepted at p<0.05. Results: Among 7155 patients, 7,155 patients met the inclusion criteria. The mean age was 61.5 years. Of this cohort, 1,031 (14.4%) had at least one lymph node evaluated. There was no difference in age or gender. Multivariate logistic regression showed that the LND group was more likely to have had postoperative blood transfusion (p < 0.001), longer operative time (p < 0.001), and less likely to be planned laparoscopic/robotic (p < 0.001). Conclusions: Prior studies have failed to demonstrate significant benefit of nephrectomy plus LND versus nephrectomy alone. Here, we present evidence that performing LND in conjunction with nephrectomy increases the risk of postoperative transfusion requirement. Although the role of LND in RCC is uncertain, the potential for these complications should factor into risk-benefit analysis when deciding whether to perform LND for patients with RCC especially in patients with high bleeding risk. SOURCE OF Funding: N/A