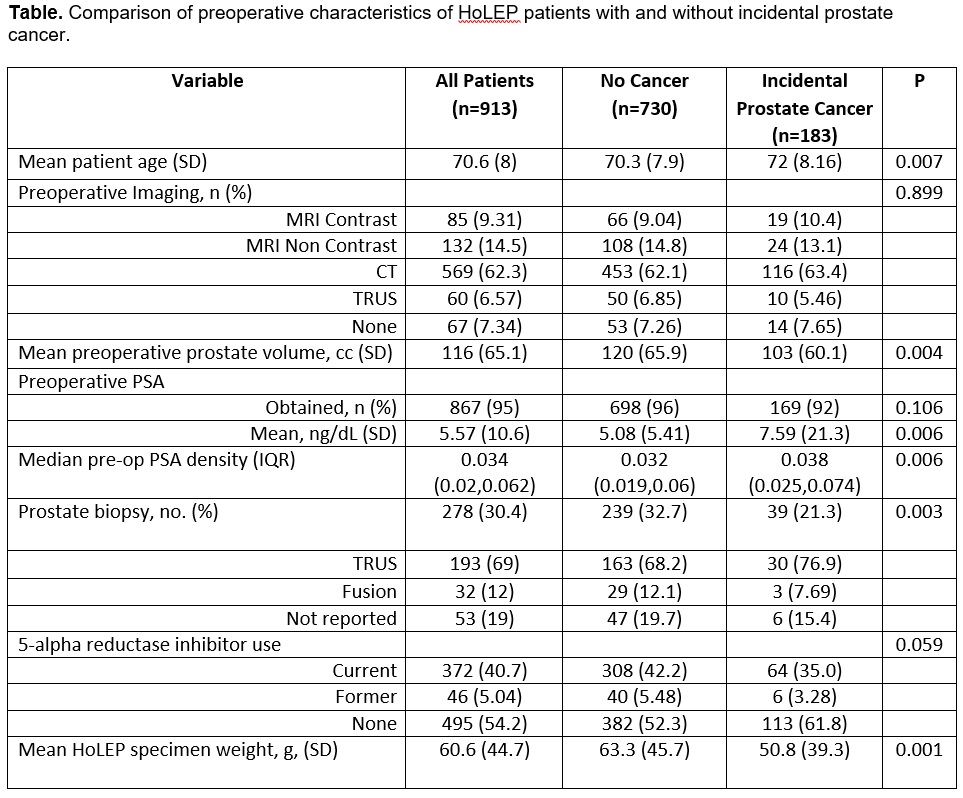
Introduction: The published rate of incidental prostate cancer detection (iPCa) after holmium laser enucleation of the prostate (HoLEP) is widely variable from 7-23%. We aim to determine the incidence and risk factors associated with iPCa diagnosis to inform development of a prospective, risk stratified approach to preoperative evaluation for concomitant prostate cancer prior to HoLEP. Methods: Consecutive patients undergoing HoLEP from 2018-2022 were included and comprehensive clinical data abstracted from a prospectively maintained database. Patients with known diagnosis of prostate cancer prior to HoLEP were excluded (n=31). iPCa was defined as a diagnosis of PCa on pathologic examination of the HoLEP specimen. Patients with and without iPCa were compared with respect to pre-operative clinical variables using Chi-square and Wilcoxon rank sum tests. Association of clinical variables with diagnosis of iPCa were assessed using logistic regression. Results: We included 913 patients in the analysis. The majority of patients (95%) had a pre-operative PSA, 9% had negative MRI, and 30% had negative prostate biopsy (Table). 183 (20%) patients were diagnosed with iPCa. The majority of cancers were cT1a (84%) and grade group 1-2 (87%). Patients diagnosed with iPCa were significantly older, had smaller prostate volume, higher PSA, and were less likely to have preoperative prostate biopsy (Table). On multivariable analysis, PSA density (OR 1.06 95% CI 1.02, 1.1), preoperative biopsy (OR 0.549, 95% CI 0.332, 0.908), and HoLEP specimen weight (OR 0.994, 95% CI 0.989, 0.999) were significantly associated with iPCa diagnosis. Conclusions: In a significantly pre-screened population, we identified a 20% incidence of iPCa after HoLEP. Risk factors for iPCa diagnosis included increasing PSA density, lower specimen weight, and not having a preoperative biopsy. In the future, we propose more rigorous and risk-stratified preoperative screening in this unique patient population. SOURCE OF Funding: None

 photo")