PD10-06: A Nomogram to Predict Lymphnode Involvement in Candidates to Robot-Assisted Radical Prostatectomy with iT3 Prostate Cancer on Preoperative Multiparametric MRI as Unique High-Risk Feature
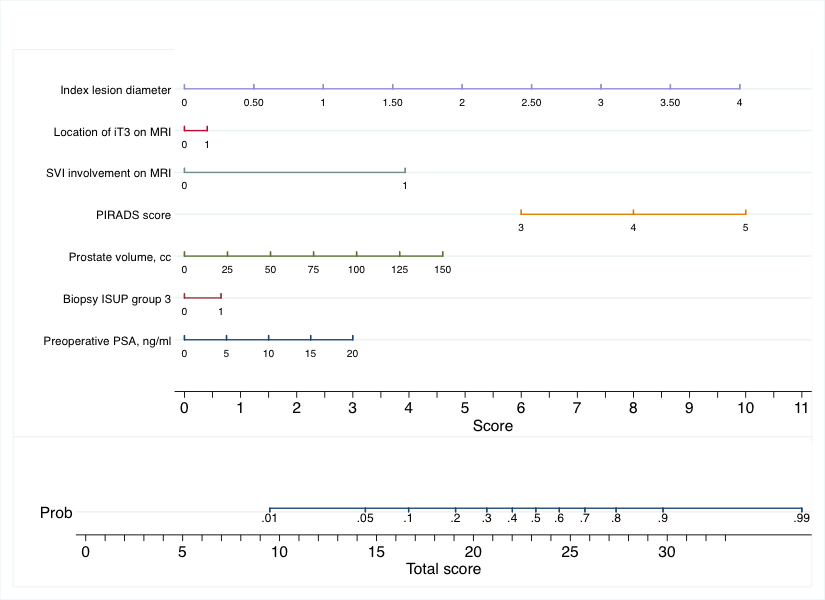
Introduction: Patients diagnosed with locally advanced prostate cancer (PCa) on preoperative MRI (iT3) are automatically included in the high-risk category. However, we previously showed that 1 in 3 men with iT3 PCa had pT2 disease on final pathology. As such, if iT3 disease is the only high-risk feature in candidates to robot-assisted radical prostatectomy (RARP), it might mislead preoperative counselling, especially when an extended pelvic lymph node dissection (ePLND) in contemplated. Therefore, we assessed predictors of pathologic lymphnode involvement (LNI) in the largest series of men with iT3 PCa treated with RARP. Methods: We analyzed data of 607 patients with iT3 PCa who received RARP and ePLND at five high-volume centers between 2015 and 2020. Among them, 253 (42%) men had iT3 disease as unique feature of high-risk PCa. In this subgroup of patients, multivariable regression investigated preoperative predictors of LNI on final pathology, namely preoperative PSA, biopsy grade, prostate volume on MRI, index lesion PIRADS score and diameter, location suspicious for iT3 (uni- vs. bi-lateral) and seminal vesicles involvement on MRI. The coefficients were utilized to build a nomogram for the prediction of LNI. Results: Median (interquartile range [IQR]) preoperative PSA was 7.2 (5.0, 10.8) ng/ml, and 42 (17%), 106 (42%) and 105 (42%) men had biopsy ISUP group 1, 2 and 3 disease, respectively. A total of 142 (56%) patients had a PIRADS score 5 lesion, whereas the median (IQR) index lesion diameter was 1.8 (1.3, 2.9) centimeters. After surgery, a total of 40 (16%) patients had LNI on final pathology. The role of preoperative predictors was investigated on multivariable logistic regression analysis, and coefficients were utilized to build a nomogram for the prediction of LNI on final pathology (Figure 1). The area under the curve was 71% (95% confidence interval: 62%, 79%). Conclusions: In the largest series of candidates to RARP with iT3 PCa as unique high-risk feature, we developed an easy-to-use model for the prediction of LNI on final pathology. The nomogram-derived probability can help physicians to optimize surgical strategy in this subgroup of patients with preoperative imaging suggesting iT3 PCa. SOURCE OF Funding: None