Hospital das Clinicas, Faculdade de Medicina da Universidade de Sao Paulo AND Memorial Sloan Kettering Cancer Center
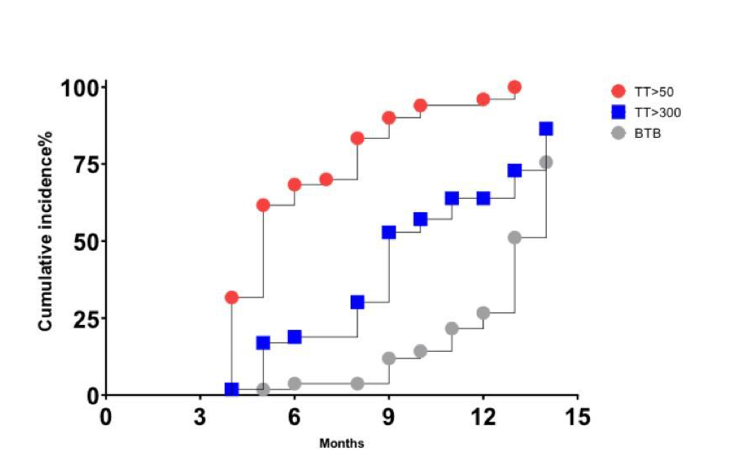
Introduction: Testosterone (T) recovery after androgen deprivation therapy (ADT) is reported variably in the literature (7 to 96%), due to variable definitions, follow up periods and with data coming mainly from restrospective studies. Age, diabetes and baseline T are reported as associated factors with recovery. Our aim was to report the chronology of T recovery following ADT cessation Methods: This is a secondary analysis of an oncological study with a prospective design evaluating the neoadjuvant use of ADT in combination with abiraterone acetate and prednisone with or without apalutamide in high-risk localized patients. Both regimens were administered for 3m before radical prostatectomy (RP). Early morning Total T (TT) levels were collected at baseline and periodically (3, 6 and 12 m) after ADT cessation. 3 outcomes for T recovery were evaluated: return to non-castrate level (TT >50 ng/dL), to normal (TT = 300 ng/dL) and back to baseline level (BTB –TT= baseline level). We performed a time-to-event analysis and reported the cumulative incidence of each outcome. Multivariable analysis was conducted to investigate predictors of recovery Results: In this preliminary report, from 64 initially enrolled patients, 1 year follow-up T data from 50 pts were available. Mean age was 64,6y (± 5,89), 28% had type 2 diabetes (DM) and 61% hypertension (HTN). Mean baseline TT was 450ng/dl ( ± 170) ng/dL, 112,7 at 3m ( ± 96,9), 208,5 ( ±197) at 6m, 337,7 ( ± 170) at 9m and 378,2 (± 166) at 12 m. Figure 1 represents the cumulative incidence of each outcome according to time. Median time to achieve T>50 was 5 m, to achieve T>300 was 9,1m and BTB 13,13 m. At 1 year, 98% had return back from castrate-level, 76% had TT normalized and only 42% had return BTB. In multivariable analysis including DM, HTN, age and baseline T, only baseline T was significantly associated with a greater chance of recovery, with 88,5% and 46,9% achieving normal T at 1y for patients with baseline T greater and lower than 450 ng/dl (HR: 3,56, p=0,0008) Conclusions: In this prospective analysis of a population exposed to neoadjuvant short-term ADT, T recovery rates were relatively high at1 year, with 98% having TT>50ng/dl, about 2/3 third having TT back to TT>300ng/dl, but with less than half with BTB level. An effort should be made to measure TT before starting ADT SOURCE OF Funding: Janssen-Cilag Farmace^utica Ltda