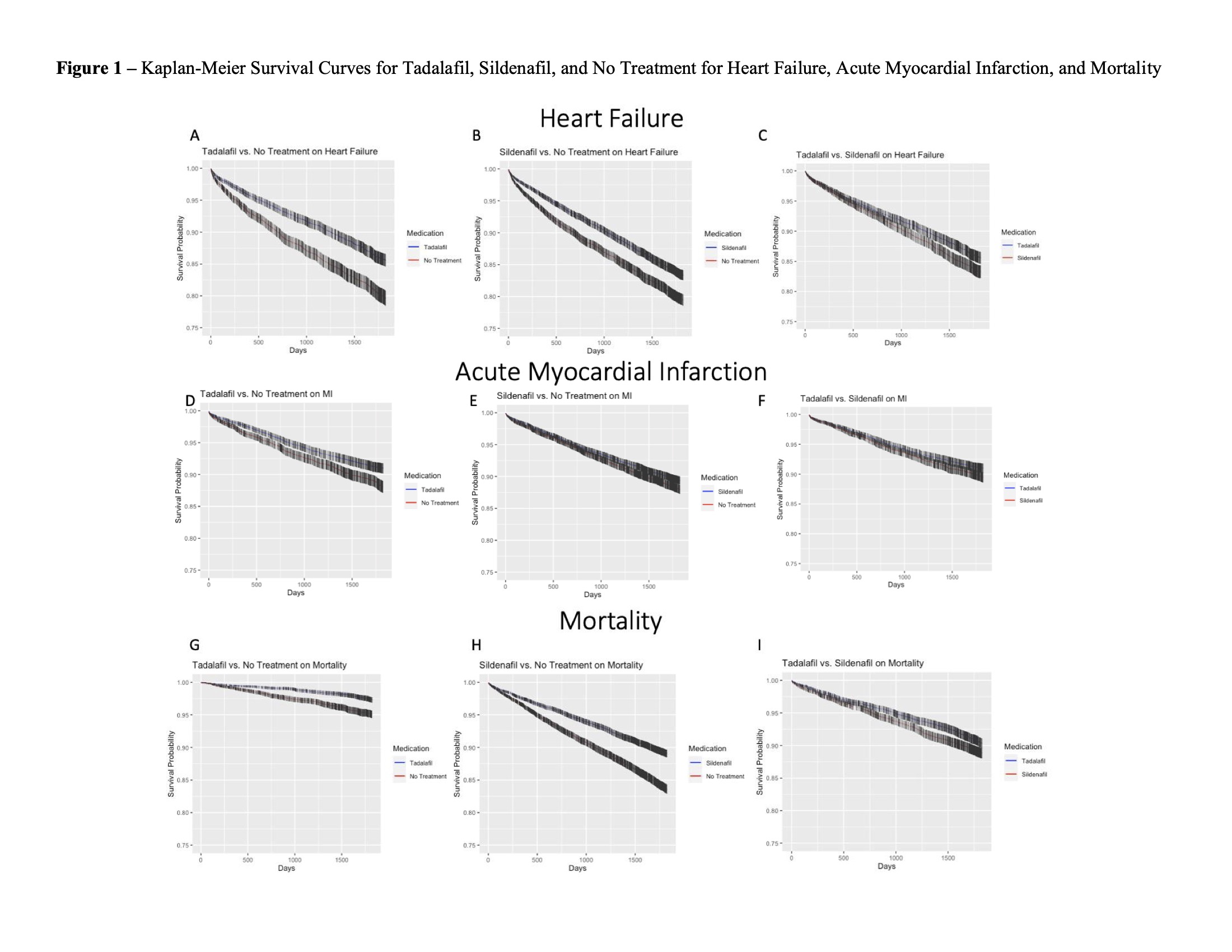
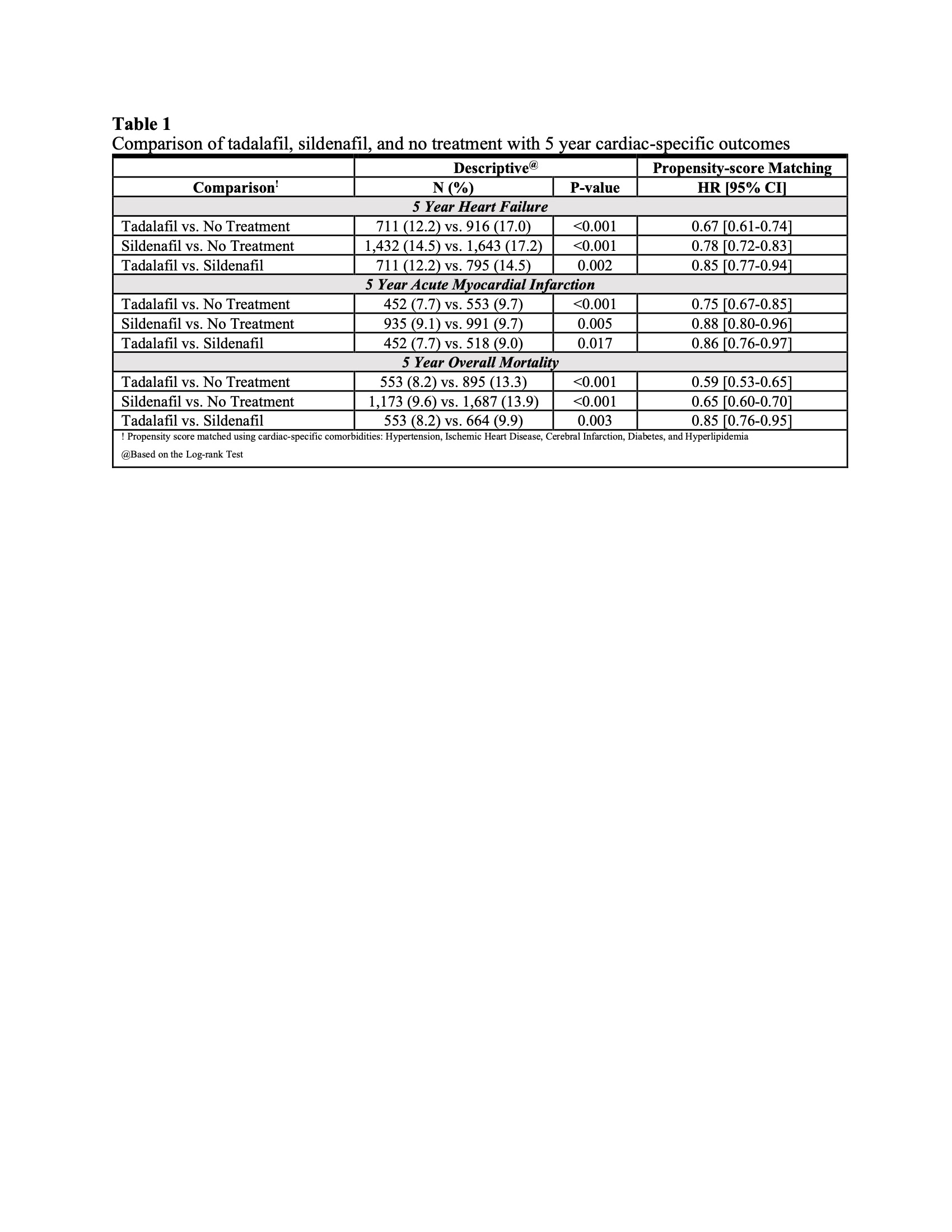
Introduction: Coronary artery disease (CAD) and erectile dysfunction (ED) often co-occur due to shared vascular risk factors. Although phosphodiesterase-5-inhibitors (PDE5i) are first line treatments for ED, they have also been shown to improve myocardial perfusion and cardiac contractility. To date, information regarding PDE5i and their perceived cardiac benefits has been limited. We hypothesized that tadalafil, with its high affinity to PDE5 receptors compared with sildenafil, may provide greater clinical benefits in reducing major adverse cardiac events (MACE). Methods: A retrospective, propensity-matched cohort study was performed using the TriNetX Research Network. Patients with ICD-10 codes for CAD and ED but not pulmonary hypertension were captured (1/2011-12/2016). Patients were subdivided and analyzed via pairwise fashion according to known prescriptions for tadalafil (T), sildenafil (S), or no treatment (NT). Propensity matching was performed using baseline comorbidities of hypertension, ischemic heart disease, cerebral infarction, diabetes, and hyperlipidemia. Outcomes of interest included 5-year rates of heart failure (HF), acute myocardial infarction (MI), and mortality. Results: A total of 41,287 male patients were identified, with 6,751 with concurrent tadalafil use, 12,214 with sildenafil use, and 22,321 with NT. When compared with NT, both tadalafil and sildenafil were associated with reduced progression to HF, MI, and overall mortality (Figure 1). Most importantly, compared with sildenafil, tadalafil demonstrated lower progression to HF (HR: 0.85 [0.77-0.94]), MI (HR: 0.86 [0.76-0.97]) and mortality (HR: 0.85 [0.76-0.95]) (Table 1). Conclusions: Tadalafil use was associated with a significant reduction in progression to HF, MI, and mortality compared with sildenafil or no treatment. These preliminary results may signal meaningful clinical differences in drug choice for men suffering from CAD and ED, and therefore require further inquiry. SOURCE OF Funding: None