University of Wisconsin School of Medicine and Public Health
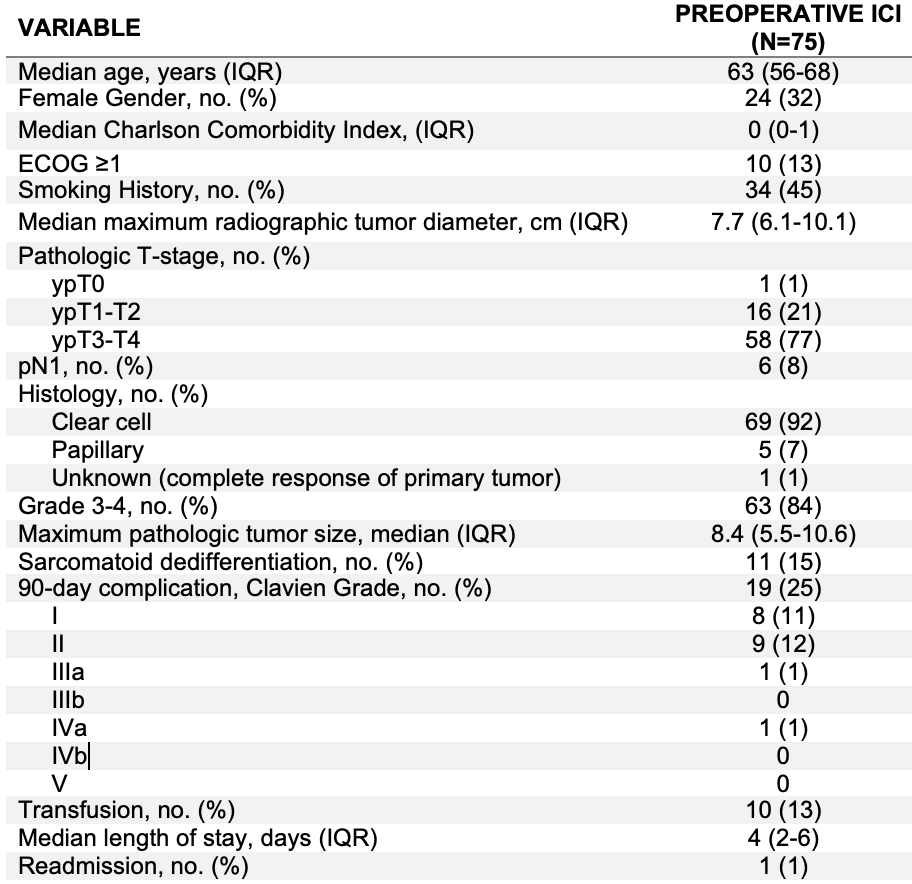
Introduction: Immune checkpoint inhibitors (ICI) are first line therapy for metastatic renal cell carcinoma (mRCC). Additionally, cytoreductive nephrectomy (CN) is often performed after initial ICI therapy. Few data exist on the effect of upfront ICI therapy on perioperative CN outcomes. This study evaluated intraoperative and postoperative CN outcomes for patients who underwent upfront ICI. Methods: Four tertiary level institutions retrospectively evaluated perioperative outcomes among consecutive patients who received upfront ICI followed by deferred CN. Intraoperative and postoperative outcomes were tabulated. Complications were graded according to the Clavien-Dindo complication scale with complications grade =III considered to be high grade. Results: A total of 75 patients were identified between 2017-2022. Clinical characteristics are listed in Table 1. The patients were generally healthy with good performance status. Majority were IMDC intermediate risk (71%) and received ipilimumab and nivolumab therapy (90%). Median time on ICI therapy was 3 months (IQR 2-9). The majority underwent an open radical nephrectomy (71%) of which 13% had an IVC thrombus. The median operative time was 177 minutes (IQR 112-239) with median blood loss of 195cc (IQR 100-400). Three patients had intraoperative complications. Median length of stay was 4 days. The 90-day complication rate was 19/75 (25%), of which only 2/75 (3%) were high grade (Clavien =III). This included one patient who aspirated and required intubation and another patient with an upper GI bleed requiring endoscopy. None died within 90 days, and 1 patient was readmitted within 30 days. Regarding postoperative therapy, 36/75 (48%) were rendered with minimal or no residual disease and have not restarted ICI therapy at last follow-up. Of those that did restart therapy, the median time to restart ICI was 34 days (IQR 23-56 days). Conclusions: In this select group of consecutive patients with good PS treated at tertiary level hospitals, deferred CN following ICI therapy was safe with rare incidence of high-grade complications. Additionally, many patients were rendered with minimal residual disease allowing them to be placed on surveillance thus avoiding the toxicity of further ICI therapy. SOURCE OF Funding: None

.jpg "Daniel Shapiro, MD (he/him/his) photo")