Consultant Urologist Sapienza University of Rome, Italy
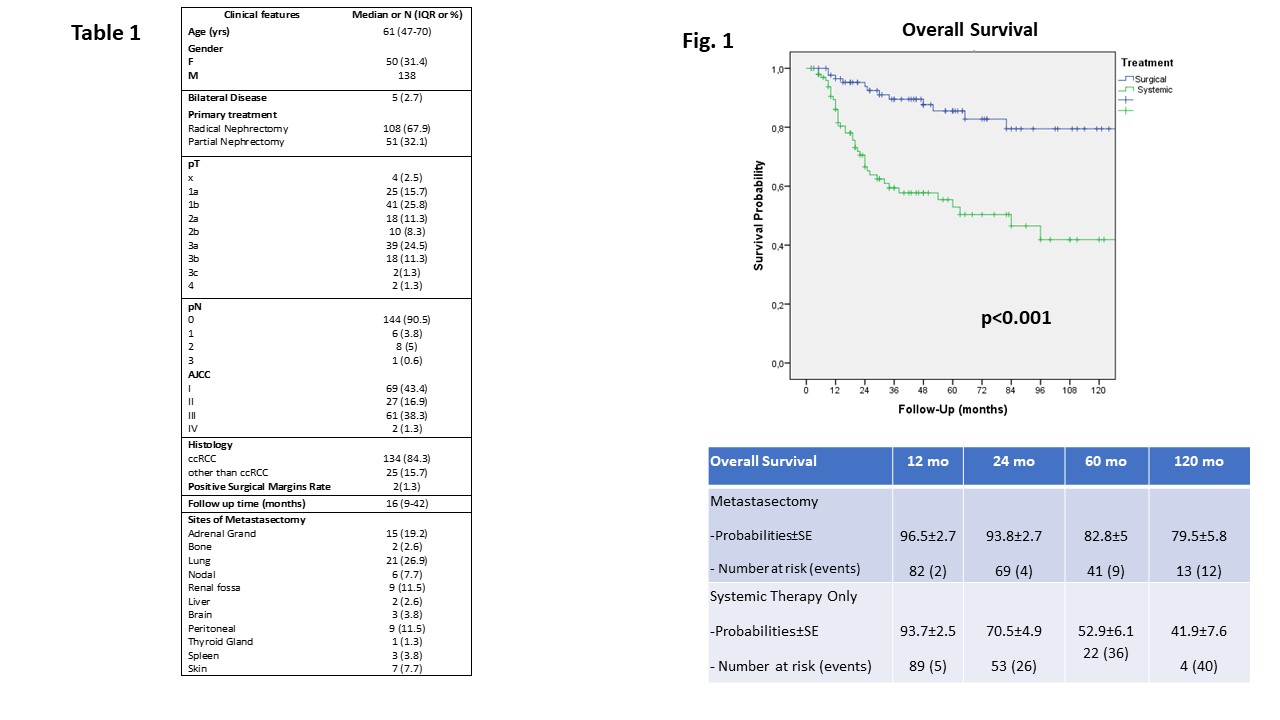
Introduction: Solitary or oligometastasis from renal cell carcinoma (RCC) are considered the ideal candidate for target treatments to delay the time to systemic therapies. The role of surgical metastasectomy and its impact on survival outcomes remains poorly addressed. We evaluated the impact of mestastasectomy on overall survival in patients with oligometastatic (m) RCC. Methods: Institutional renal cancer prospective database was queried for cases treated with partial or radical nephrectomy who developed metastatic disease during follow up. Patients with evidence of clinical metastasis at first diagnosis were excluded. Patients were unfit for metastasectomy based on surgeon's discretion (not achievable a non evident disease [NED] status after surgery), all other patients received systemic treatment. Survival probabilities were computed at 12, 24, 60 and 120 months after primary treatments. The impact of metastasectomy vs systemic treatment only cohort (reference category) was assessed with the Kaplan Meier method. Age, gender, bilaterality, histology, AJCC stage of primary tumor, surgical margins and metastasectomy were included in univariable and multivariable regression analyses to assess predictors of overall survival (OS). Results: Overall, at a median follow up of 16 months after primary treatment, 168 patients with RCC developed asynchronous metastasis at adrenal gland, lung, liver, spleen, peritoneal, renal fossa, bone, nodes, brain and thyroid gland. Nine patients unfit for any treatment were excluded. The site of metastasis was treated with surgical metastasectomy (77/159, 48.4%), with or without previous or subsequent systemic treatment (table 1), while 82/159 cases (51.2%) received only systemic treatment. Two-yr, 5-yr and 10-yr overall survival probabilities were 82.9%,72%, 62.7% respectively. At multivariable analysis, primary tumor AJCC stage and metastasectomy were independent predictors of OS probabilities (p=0.009 and <0.001, respectively). At Kaplan Meier analysis, metastasectomy improved significantly OS probabilities versus patients receiving systemic therapy (p < 0.001). (Fig.1) Conclusions: When a NED status is achievable, surgical metastasectomy of mRCC significantly impact on OS delaying and not precluding further subsequent systemic treatments. SOURCE OF Funding: None