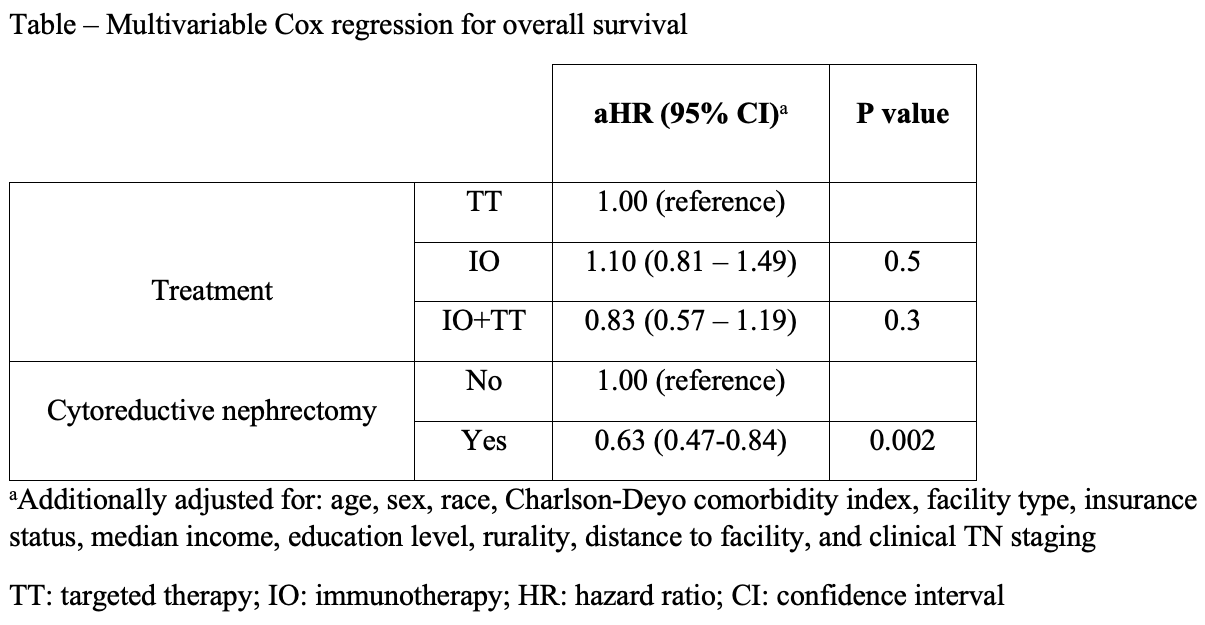
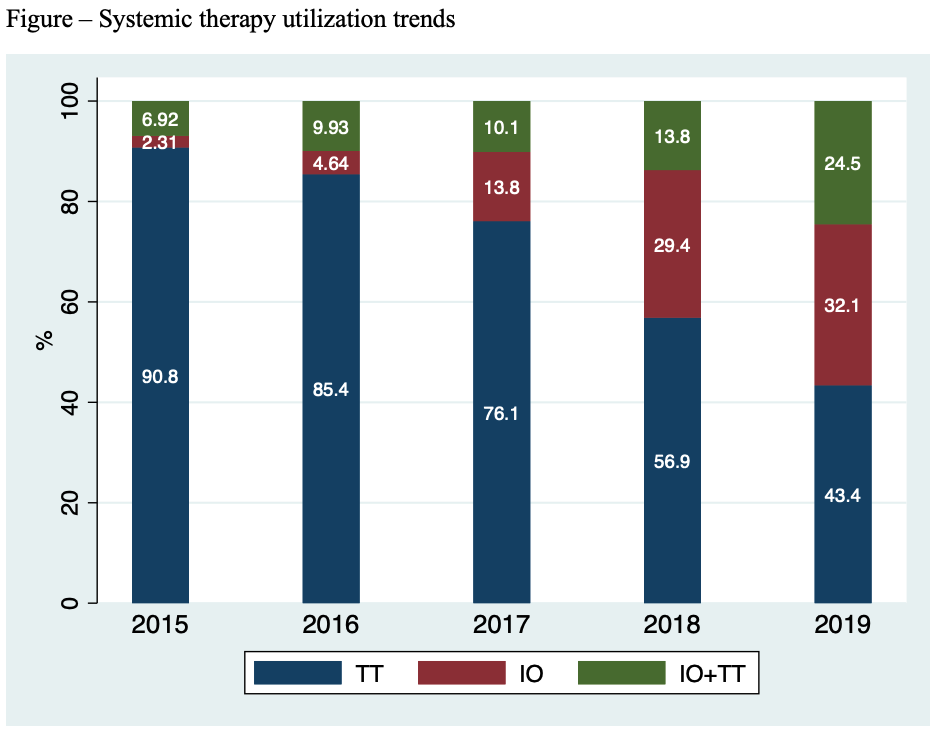
Introduction: Much of the data used to advise patients with metastatic papillary renal cell carcinoma (pRCC) is derived from studies in the setting of metastatic clear cell renal cell carcinoma (ccRCC). The current standard of care for patients with metastatic ccRCC is immunotherapy (IO) with or without targeted therapy (TT). Except for a few phase II randomized clinical trials, the benefit of IO or IO+TT combination has not been thoroughly explored in metastatic pRCC. We sought to describe real-world utilization trends of TT, IO, and IO+TT and their impact on overall survival (OS) in the setting of metastatic pRCC with or without cytoreductive nephrectomy (CN). Methods: We queried the National Cancer Database (NCDB) to identify adult patients with de novo metastatic pRCC who had received first-line TT, IO, or IO+TT. The primary outcomes of interest were trends in systemic therapy utilization and OS benefit. We performed multivariable Cox proportional hazards regression analysis to evaluate the association between the type of systemic therapy and OS, after adjusting for receipt of CN and other covariates. Results: A total of 737 patients with metastatic pRCC were identified: 512 (69.5%), 126 (17.1%), and 99 (13.4%) had received TT, IO, and IO+TT, respectively. The proportion of patients who received IO and IO+TT increased steadily during the study period. After adjusting for baseline differences, CN was associated with a benefit in OS (HR 0.63, 95% CI 0.48-0.84). However, neither IO (HR 1.10; 95% CI 0.81-1.49) nor IO+TT (HR 0.83, 95% CI 0.57-1.19) were associated with better OS compared to TT alone. Conclusions: In patients with metastatic pRCC, neither IO or IO+TT were associated with an improvement in OS, compared to TT alone. SOURCE OF Funding: N/A

 photo")