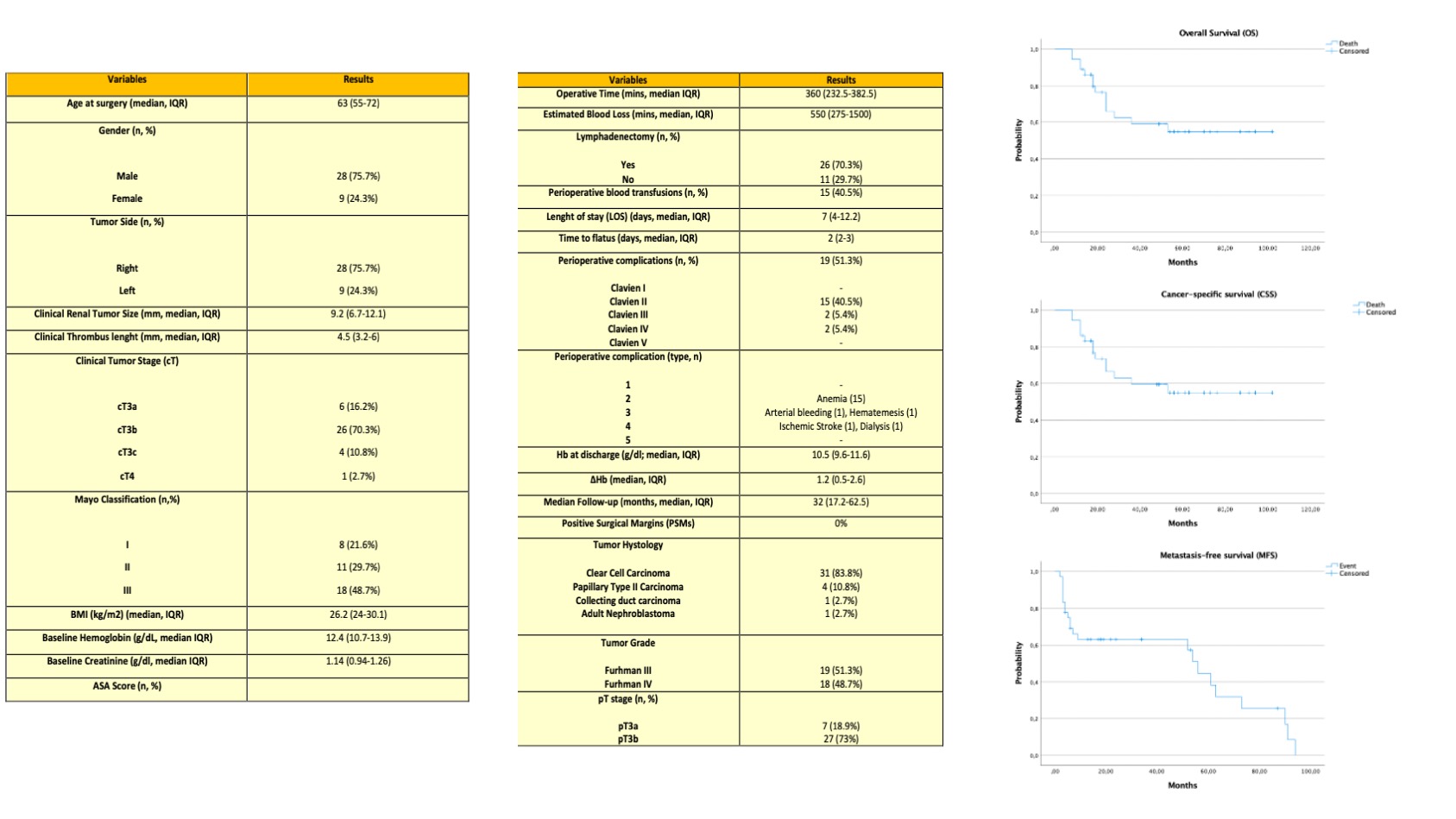
Introduction: Few series of robot-assisted radical nephrectomy (RARN) with inferior vena cava tumor thrombectomy (IVCT) for renal cell carcinoma (RCC) with venous tumor thrombus (VTT) are available in literature, all with short-term oncologic outcomes. The aim of this study is to describe perioperative and long-term oncologic outcomes of RARN and IVCT performed at a single, high-volume centre. Methods: Between January 2014 and October 2022, 37 consecutive patients underwent RARN-IVCT for RCC and VTT at a single tertiary-care center. Baseline, demographic and perioperative data were collected. A descriptive statistical analysis was performed. Frequencies and proportions were reported for categorical variables while medians and interquartile ranges (IQRs) were reported for continuously coded variables. Overall survival (OS), disease-free survival (DFS) and metastasis-free (MFS) were computed with the Kaplan-Meier method. Results: Overall 37 consecutive patients were included in the analysis, 8 with VTT Mayo level I (21.6%), 11 with level II (29.7%), and 18 with level III (48.7%), respectively. All cases were successfully completed without conversion to open surgery. Median operative time was 360 minutes (IQR 232.5-382.5). Median estimated blood loss was 550 ml (IQR 275-1500). Median hospital stay was 7 days (IQR 4-12.2). Overall, 19 patients (51.3%) had perioperative complications, 15 Clavien grade 2 (40.5%, all blood transfusions) and 4 grade 3-5 (10.8%), respectively. At a median follow-up of 32 months (IQR 17.2-62.5), MFS, DFS and OS probabilities were 37.8%, 59.4%, and 59.4%, respectively. The small series, the high rate of adjuvant targeted therapies (32.4%) as the extreme surgical complexity may affect reproducibility of outcomes. Conclusions: RARN-IVCT represents a feasible and safe surgical option in tertiary referral centers; mid-term oncologic results seem to be comparable to those reported in open surgery literature. Our results support RARN-IVCT as a feasible and safe surgical option in tertiary referral centers even in the most advanced setting. SOURCE OF Funding: None