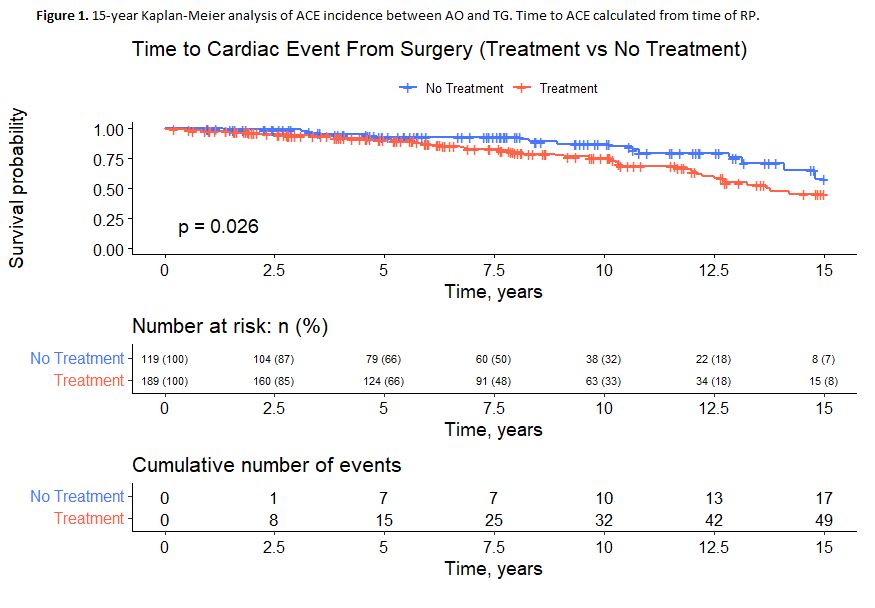
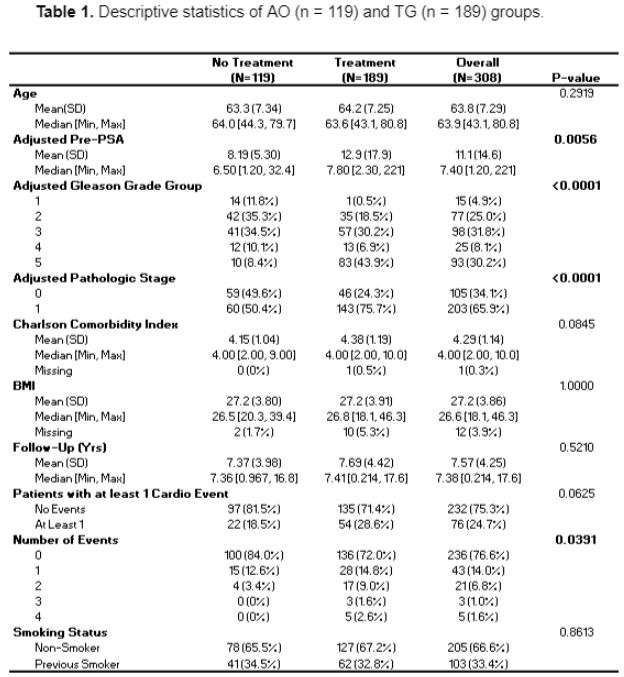
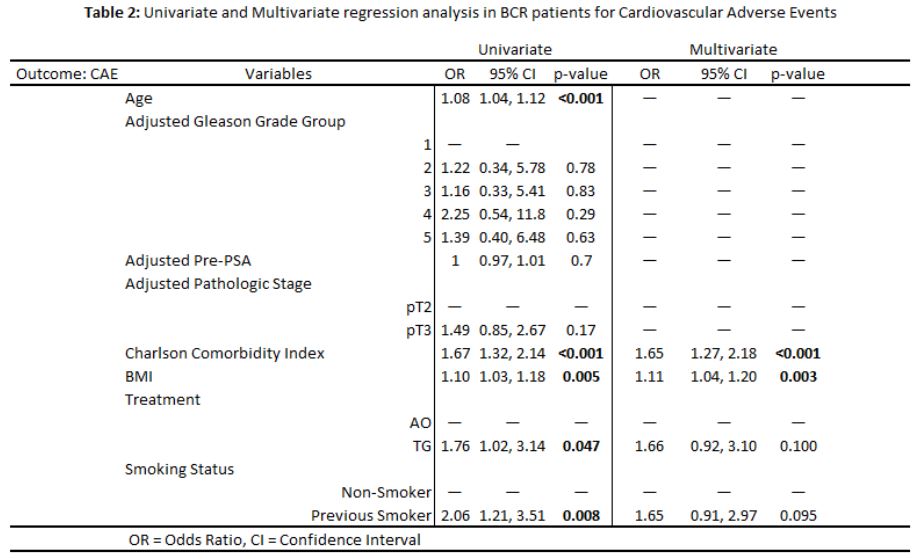
Introduction: Androgen deprivation therapy (ADT) is frequently recommended for biochemical recurrence (BCR) following a radical prostatectomy (RP). The most severe life-threatening complication of ADT is an adverse cardiovascular event (ACE) such as acute myocardial infarction, stroke, etc. There exists a conflict between the relationship of PC, ADT and ACEs in the literature. This study seeks to assess the relationship of ACE and cardiovascular mortality (CM) in men undergoing ADT post-RP. Methods: Retrospective review of prospectively collected data (n = 1895) from patients who underwent robot-assisted radical prostatectomy (RARP) performed by a single surgeon. 308/407 with BCR and adequate follow-up data were analyzed. 189/271 men in the “treatment group” (TG) were managed with ADT. The comparator group was 119/136 with no treatment (AO). Regression and Kaplan Meier (KM) analyses were performed. Results: At time of surgery, there were no significant differences in Charlson comorbidity index (CCI) but a trend in favor of AO (4.14 versus 4.38; Table 1). Significant predictors of ACEs in univariate analysis were age, CCI, body mass index (BMI), treatment status (AO vs TG), and smoking status (non-smoker vs previous smoker; Table 2). 15-year KM analysis showed a statistically significant increase in ACEs (TG 54.4% and AO 41.8%, p = 0.02; Figure 1). In adjusted analysis, CCI and BMI were significant predictors for ACE with treatment trending toward significance. No differences in CM were observed. Conclusions: Although BCR was associated with increased acute cardiovascular events, remarkably this was not observed in CM. We also noted the importance of BMI and CCI as a prognosticating tool for predicting acute cardiovascular events. SOURCE OF Funding: N/A