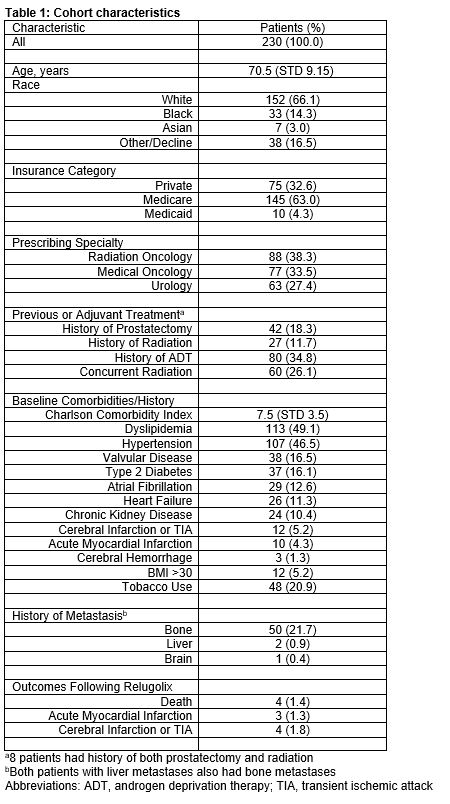
Introduction: Relugolix is an oral GnRH antagonist that was FDA approved in December of 2020 which causes rapid testosterone suppression and rebound upon discontinuation, and potentially decreases androgen deprivation therapy related cardiovascular events. We sought to determine the characteristics and cardiovascular outcomes of patients with prostate cancer treated with relugolix at our institution. Methods: The Northwestern Electronic Data Warehouse was queried for men with an established diagnosis of prostate cancer for whom relugolix was prescribed between December 2020-July 2022. Baseline clinicopathologic characteristics, cardiac health information, Charlson comorbidity index (CCI), and cardiac outcomes following initiation of relugolix were collected. Results: 230 men (mean age 70.5 years) were prescribed relugolix at our institution. Relugolix was most commonly prescribed by radiation oncology (38.3%, n=88), followed by medical oncology (33.5%, n=77), and urology (27.4%, n=63). Patients had high CCI (mean 7.5) and 69.1% had a history of cardiovascular disease or at least one cardiovascular disease risk factor prior to initiation of therapy (n= 159). The most common risk factors included history of dyslipidemia (49.1%, n=113) and hypertension (46.5% n=107). Following initiation of relugolix, 11 major adverse cardiac events, defined as non-fatal MI, non-fatal stroke, and death from any cause, were observed. Acute MI was the most common (n=3), followed by cerebral infarction (n=2) and TIA (n=2). A total of 4/230 (1.7%) patients died during the study period (n=2 cardiac arrest, n=2 other causes). Conclusions: The majority of patients who were prescribed relugolix had at least 1 cardiac comorbidity, and the subsequent rate of major adverse cardiac events was similar to the HERO registrational trial (4.8% vs 3.6%). Our findings illustrate a real-world experience of patients initiating therapy with relugolix, comorbidities present at initiation, providers managing the drug, and cardiovascular and survival outcomes following its use. SOURCE OF Funding: N/A

 photo")