PD13-07: Multiparametric MRI of the bladder as a predictive factor of histopathology at reTUR in T1GH with presence of detrusor muscle: could it have a role?
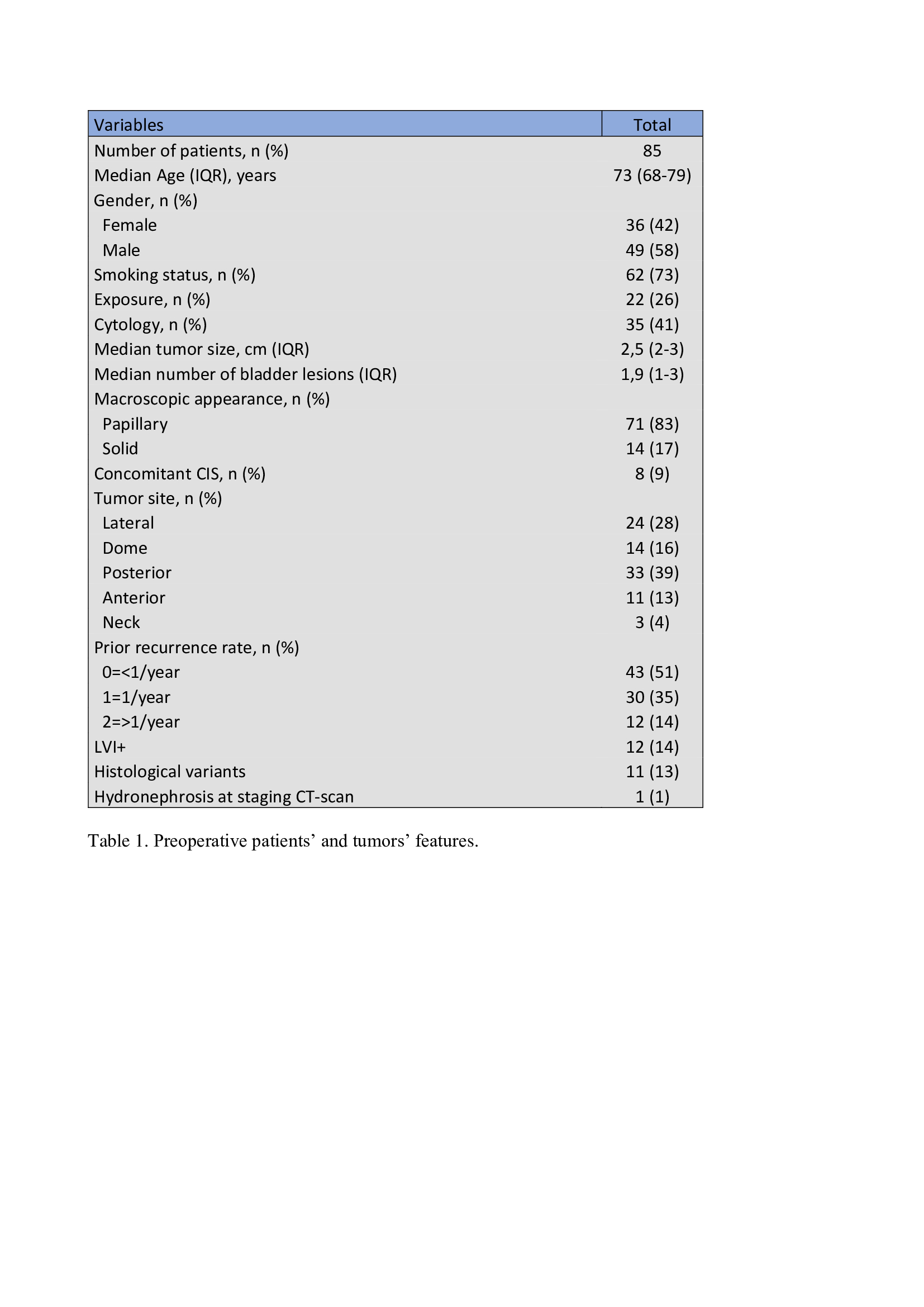
Introduction: The role of re-TUR in patients with T1 bladder tumor and muscle in TUR specimen remains controversial. Furthermore, re-TUR is an invasive procedure and a non-negligible source of logistic difficulties. On the other hand, the role of multi-parametric magnetic resonance imaging (mpMRI) for bladder cancer is growing, thanks to its high sensibility and specificity in the identification of local invasiveness of the tumor. We analyzed the role of MRI in the setting of repeated transurethral resection (reTUR) to predict absence of residual tumor (T0), persistence or understaging at first resection and we present our experience. Methods: From April 2021 to September 2022 patients with diagnosis of T1HG bladder cancer and presence of detrusor muscle at first resection underwent a bladder MRI before reTUR, after 4 or 5 weeks from the first procedure. Ethical Committee approval has been obtained. Results were classified as no evidence of residual tumor, its evidence or understaging (according to VI-RADS score). MRI was 1.5 T. Accuracy was determined using histopathology as the reference standard. Results: A total of 85 MRI was performed. 68 (80%) were classified as no residual tumor, 15 (17%) as residual tumor and 2 (3%) as suspected understaging at first resection. Accordancy with histopathology was 88%. Only in 10 (12%) cases MRI did not correctly predict results of reTUR: in 7 cases MRI classified as no residual tumors but histopathology found persistence of disease (of high grade), and 3 cases were classified as residual tumor but reTUR was negative. All 10 cases were intraoperatively macroscopically negative. The 2 cases of understaging were correctly predicted by MRI. Patients’ characteristics, tumor size, focality, site, prior recurrence rate, lymphovascular invasion, histological variants and hydronephrosis at staging CT-scan did not affect MRI accuracy. Conclusions: MRI is effective for prediction of histopathology at reTUR and could represent an effective tool in stratifying patients with T1HG who need second resection. Better instrumentation (3T-MRI), increasing experience and integration of modern prediction models can improve further our preliminary results, even including accurate cost analysis. SOURCE OF Funding: No