PD15-04: Prediction of prostate cancer specific mortality in men undergoing radiotherapy with or without hormonal treatment, risk stratification based on clinical characteristics and PSA treatment response.
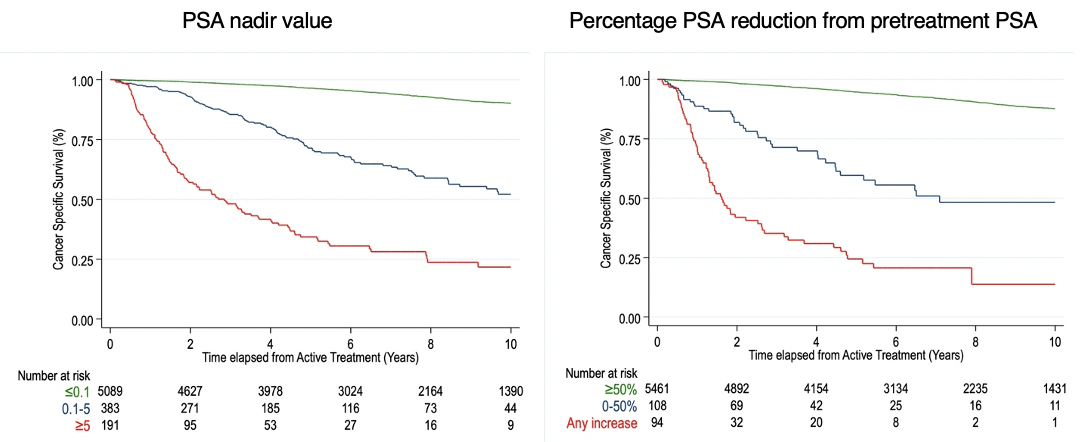
Introduction: A detectable PSA within 4 to 8 weeks of surgery is considered treatment failure post-radical prostatectomy and may result from persistent local disease, pre-existing metastases or residual benign tissue. Conversely guidelines do not mention any definition of PSA persistence after Radiotherapy (RT) with or without hormonal treatment (HT). This study aimed to evaluate if detectable PSA values after RT with or without HT predict PCa mortality and can be defined as treatment failure. Methods: This population-based study included all men in Stockholm County who underwent RT with curative intent (cM0) and PSA follow-up from 2003 to 2019. All PSA values before and after treatment were retrieved from datasets of three centralized laboratories. Results: 5663 patients were included. Median follow-up was 88 months (54, 128). HT was administered in 4457 (79%). Median time to PSA nadir was 6 (5, 21) months. 5089 (89.9%) reached a PSA nadir value =0.1 ng/ml while in 191 (3.4%) patients PSA never dropped =5 ng/ml. Median PSA reduction was 8 (5, 15) ng/ml. The percentage of PSA reduction from pretreatment PSA to nadir values was =50% in 5461 (96.4%), and <50% in 108 (1.9%). At multivariable cox regression analysis adjusting for age, pretreatment PSA, cT stage, biopsy ISUP Gleason group, HT and time to PSA nadir, we found that PSA Nadir values between 0.1-5 ng/ml (HR: 6.07; CI: 4.79,7.68) or =5 ng/ml (HR: 12.34; CI: 8.57,17.77) and percentage of PSA drop from pre-treatment PSA to nadir (HR per unit: 0.92; CI: 0.87,0.97) significantly predicted PCa-specific mortality (C-index of the model 0.82). Unadjusted cancer specific survival according to post treatment PSA nadir and percentage PSA reduction from pretreatment PSA are shown in figure 1. Similar results were found in a sensitivity analysis including patients undergoing RT without HT. Conclusions: PSA persistence and low PSA drop after RT were strongly correlated to PCa-specific mortality. A PSA nadir value >0.1 ng/ml and/or any reduction of PSA nadir <50% of pretreatment PSA values may be considered a treatment failure after RT with or without HT. Predictive models including these parameters may be used to assess the need for early treatment intensification after RT. SOURCE OF Funding: This research was supported by a grant of the European Urological Scholarship Programme awarded to U.G.F.