PD15-06: Systematic Prostate Biopsy with Insufficient Biopsy Core Number at Diagnosis Leads PSA Failure after Brachytherapy as Monotherapy for Clinical Stage T1c Prostate Cancer
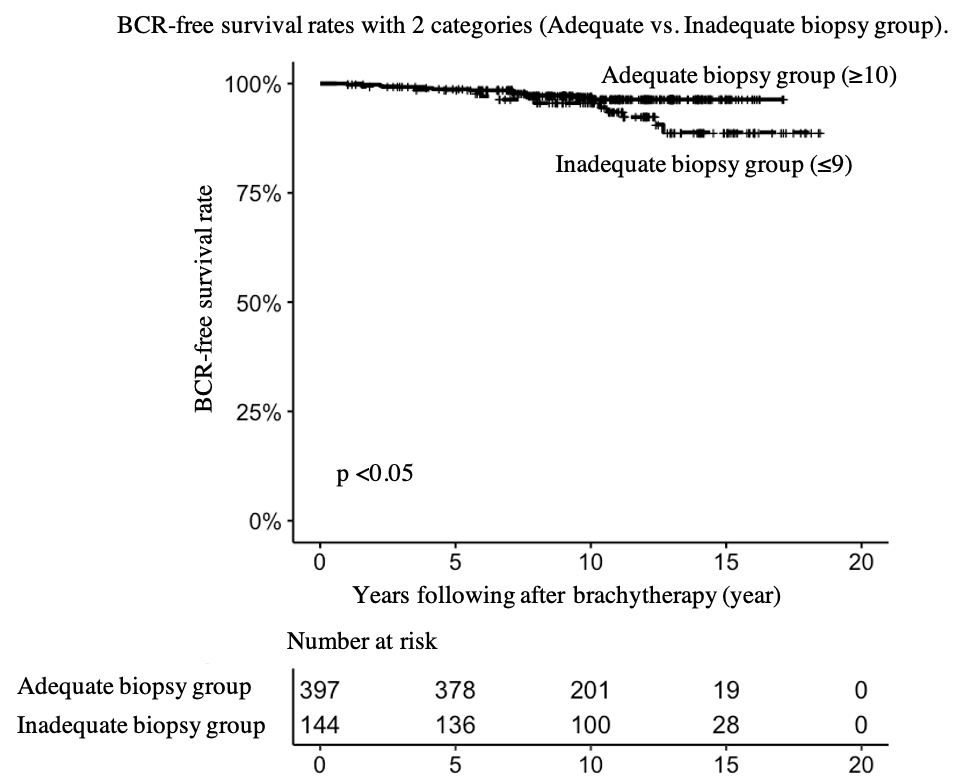
Introduction: According to the American Urological Association (AUA) guideline, systematic 10–12-core biopsy is optimal for detecting clinical stage T1c (cT1c) prostate cancer (PCA) and also for obtaining higher pathological concordance. Smaller number of prostate biopsy (PB) cores can underestimate pathological characteristics of PCA. This study reviews association between number of biopsy cores at diagnosis and clinical outcomes after low dose rate permanent seed implantation brachytherapy with iodine-125 (LDR) monotherapy. Methods: This single-institution retrospective study included 542 cT1c PCA with Gleason score 3+3=6 or 3+4=7 treated between September 2003 and September 2014 with LDR monotherapy without hormonal therapy. Local extent of disease was evaluated by digital rectal examination and pelvic MRI. All specimens of ultrasound guided trans-rectal or trans-perineal systematic PB were reviewed by urological pathologists in our institute. We statistically analyzed with Kaplan-Meier and compared rate of biochemical-recurrence (BCR)-free survival, using the Phoenix definition, between adequate (= 10 biopsy cores, N=397) and inadequate (= 9 biopsy cores, N=144) biopsy groups. Possible risk factors for BCR, such as PSA, Gleason score, biopsy core number and positive biopsy core rate, were analyzed. Results: The median age was 66 (38–87) years old and median follow up period was 10.6 (1.0–18.5) years. The median number of biopsy cores was 12 (4–46). In the adequate biopsy group, more patients had Gleason score 3+4=7 (31% vs. 15%, p <0.01). The 5- and 10-year rates of BCR-free survival rates in the adequate biopsy group were 98.7% and 96.9%, respectively, while those in the inadequate biopsy group were 98.6% and 95.6%, respectively. BCR-free survival rate was significantly higher than in the inadequate biopsy group (p <0.05). In multivariate analysis, biopsy core number =10 (Hazard ratio; HR 2.58, p <0.02) and Gleason score 3+4=7 (HR 3.26, p <0.01) were the significant factors for BCR. Conclusions: Systematic PB with sufficient core number greater than 9 leads to lower BCR in LDR monotherapy. Number of biopsy cores on PB might be an important factor for treatment outcomes. SOURCE OF Funding: None.