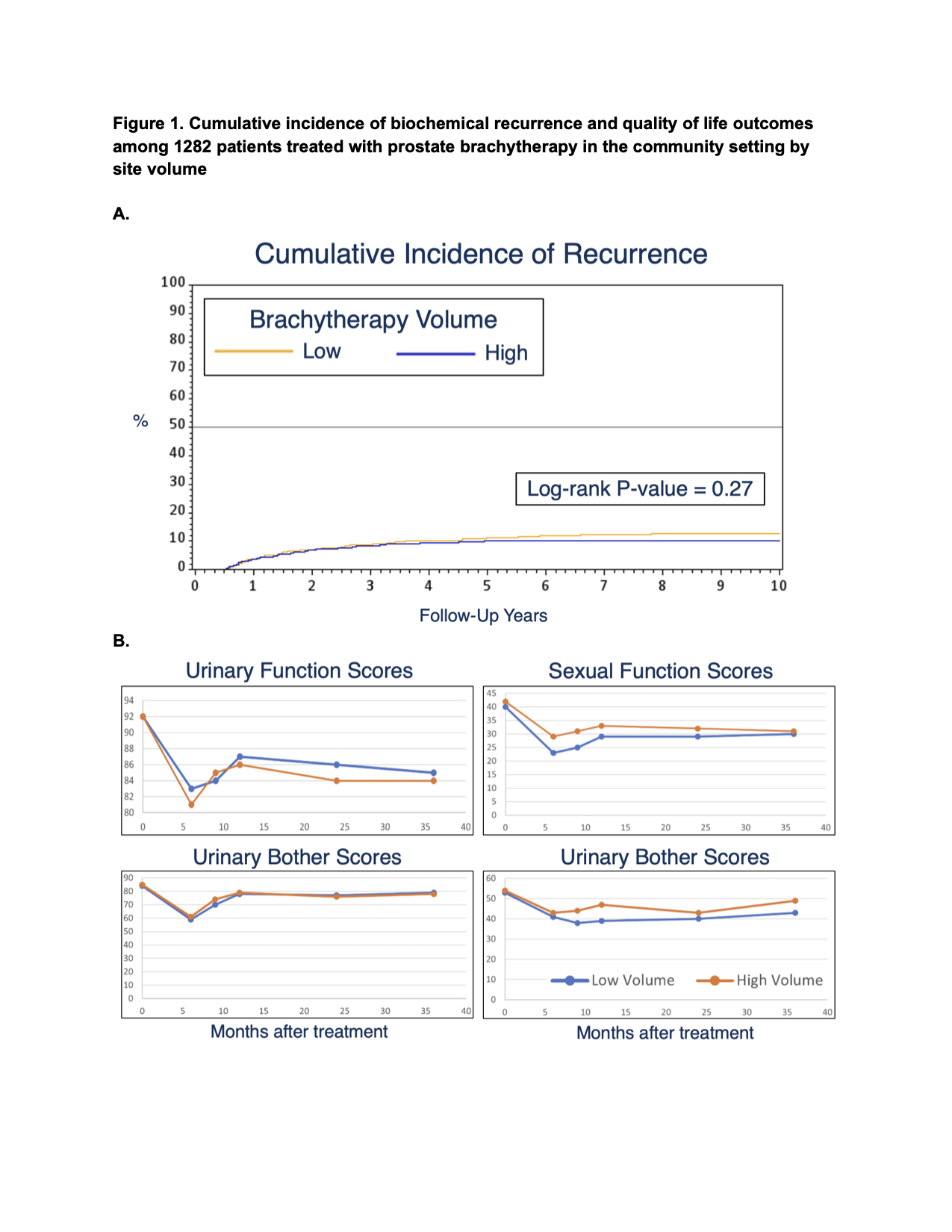
Introduction: Prostate cancer brachytherapy (BT) is a treatment modality that has been declining in usage. The goal of this study is to describe the relationship between facility BT case volume and cancer-specific outcomes in patients with localized prostate cancer (PCa). Methods: We identified patients in CaPSURE (Cancer of the Prostate Strategic Urologic Research Endeavor) diagnosed with localized PCa between 1999-2007 and treated with BT. Only community sites had sufficient recorded cases for inclusion. BT case volume of each facility was based on its number of BT-treated PCa patients, with those above the 75th percentile categorized as high-volume. Our primary outcome is the effect of case volume on biochemical failure based on the Phoenix definition or receipt of salvage treatment after primary BT to account for a large proportion of missing PSA follow-up values in our cohort. Secondary outcomes included patient-reported UCLA Prostate Cancer Index scores for urinary, sexual, and bowel function and bother. Results: We identified 1,282 BT-treated patients with localized PCa with median follow-up of 9 years (3.8 years based on last PSA) across 18 community sites with a median of 210 BT cases. Overall, 92% of patients were National Comprehensive Cancer Network low- or intermediate-risk and 98% received low dose rate BT. 722 patients (56.3%) received BT at high-volume (>210 cases) community facilities and 560 patients (43.7%) at low-volume (10-210 cases) facilities. High-volume facilities predominantly used Pd-103 seeds while low-volume facilities predominantly used I-125 seeds (p < 0.01). A greater proportion of patients at low-volume facilities had pre-BT hormone therapy (p < 0.01). High-volume facility status was not associated with improved rates of biochemical failure (10-year cumulative incidence 10.3% vs 12.5%, log-rank p=0.27, Fig. 1A) or prostate cancer specific mortality (10-year cumulative incidence 4.0% vs 4.5%, log-rank p=0.62). Patient-reported scores of urinary, sexual, and bowel bother at 6 months following BT were comparable (Fig. 1B). Conclusions: BT-treated patients with localized PCa at high-volume community facilities have similar rates of biochemical failure, prostate cancer specific mortality, and trends in quality of life outcomes compared to those treated at low-volume community facilities. SOURCE OF Funding: UCSF Goldberg-Benioff Program in Translational Cancer Biology

.jpg "Kevin Chang, BA (he/him/his) photo")