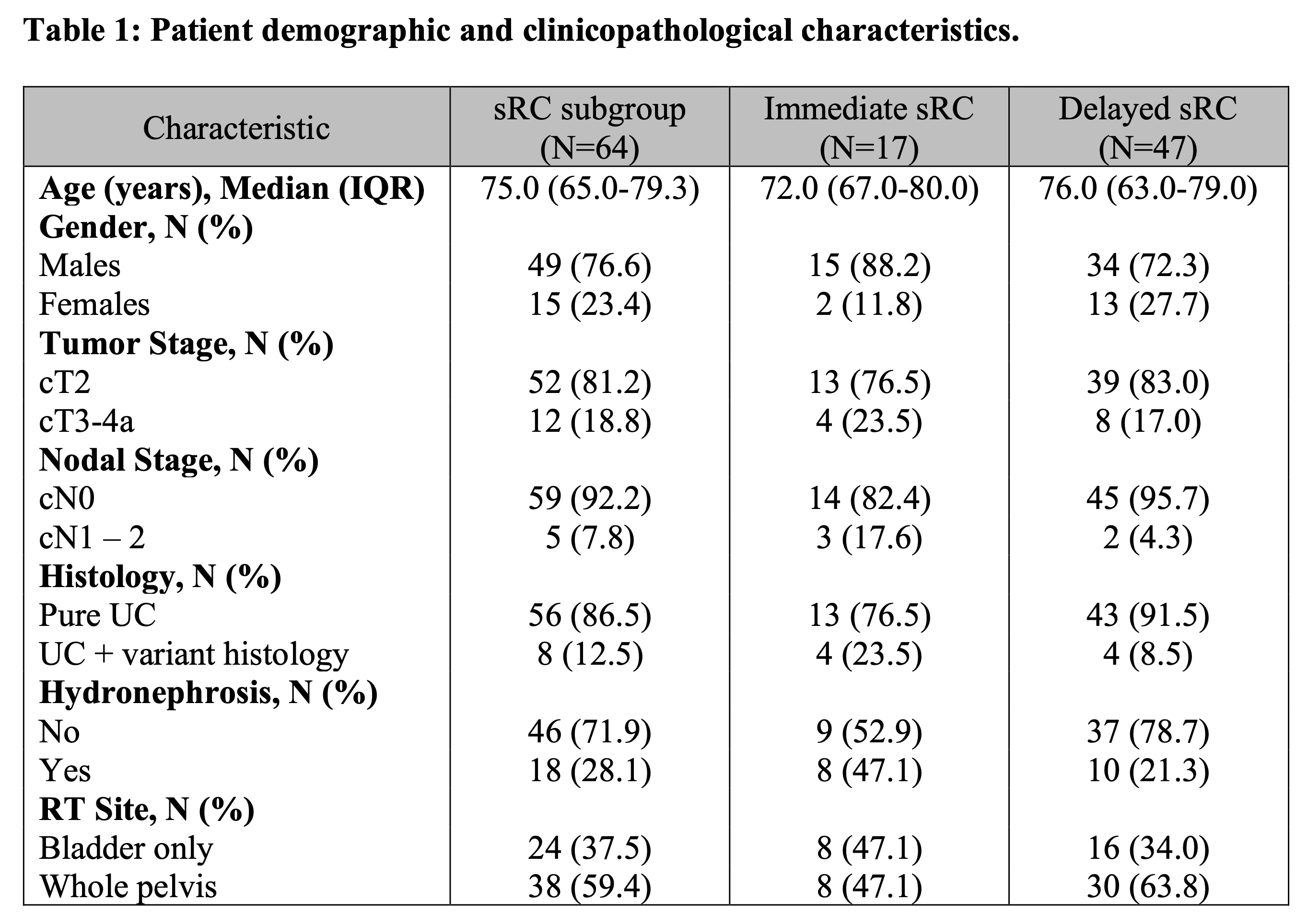
Introduction: Trimodal therapy (TMT) is an alternative to radical cystectomy for the treatment of muscle-invasive bladder cancer (MIBC) in well selected patients. Rates of recurrence and non-response to TMT have been reported to be up to 30%. Salvage radical cystectomy (sRC) is an option for patients with persistent or recurrent disease. Patient characteristics that predict success with sRC are not well defined. We report the outcomes of patients undergoing sRC from a multi-institutional Canadian cohort. Methods: Patients who underwent sRC post-TMT were identified retrospectively from the TMT Canadian Collaboration. This collaboration includes patients treated at 14 Canadian Institutions. Patient characteristics, histopathology findings, and survival outcomes were evaluated. Patients undergoing sRC were grouped into immediate (within 6 months post-TMT) and delayed sRC (more than 6 months post-TMT). Results: There were 864 patients included in this series, of which 64 underwent sRC. Of those, 17 underwent immediate sRC, and 47 delayed sRC. Patients who had an immediate salvage were more likely to be younger, male, have a higher tumor and nodal stage, variant histology, hydronephrosis and radiation to bladder only compared to those who underwent a delayed sRC (Table 1). Most patients underwent PLND (86%) with a median nodal count of 9 (4-16). Most patients underwent an ileal conduit (96.9%), and most had a negative margin (81.2%). The median overall survival (OS) for the entire cohort was 89 months. The OS between immediate and delayed sRC was 20 months and 129 months respectively. Conclusions: sRC is feasible and has acceptable oncological outcomes. Patients who undergo delayed sRC have a much better prognosis compared to those who underwent immediate sRC. This highlights the importance of patient selection when deciding between treatment options. Patients with higher T and N stage, variant histology, hydronephrosis and treated with radiation only are at an increased risk for early salvage. SOURCE OF Funding: This project has been supported by the Canadian Bladder Cancer Information System Collaborative (CBCIS) and Bladder Cancer Canada. CBCIS has received unrestricted grants or in-kind support from Bladder Cancer Canada, Merck, Roche, Astra Zeneca, Pfizer/EMD Serono, Seagen, and Bristol-Myers Squibb. There is no direct role or influence from this funding on this work.