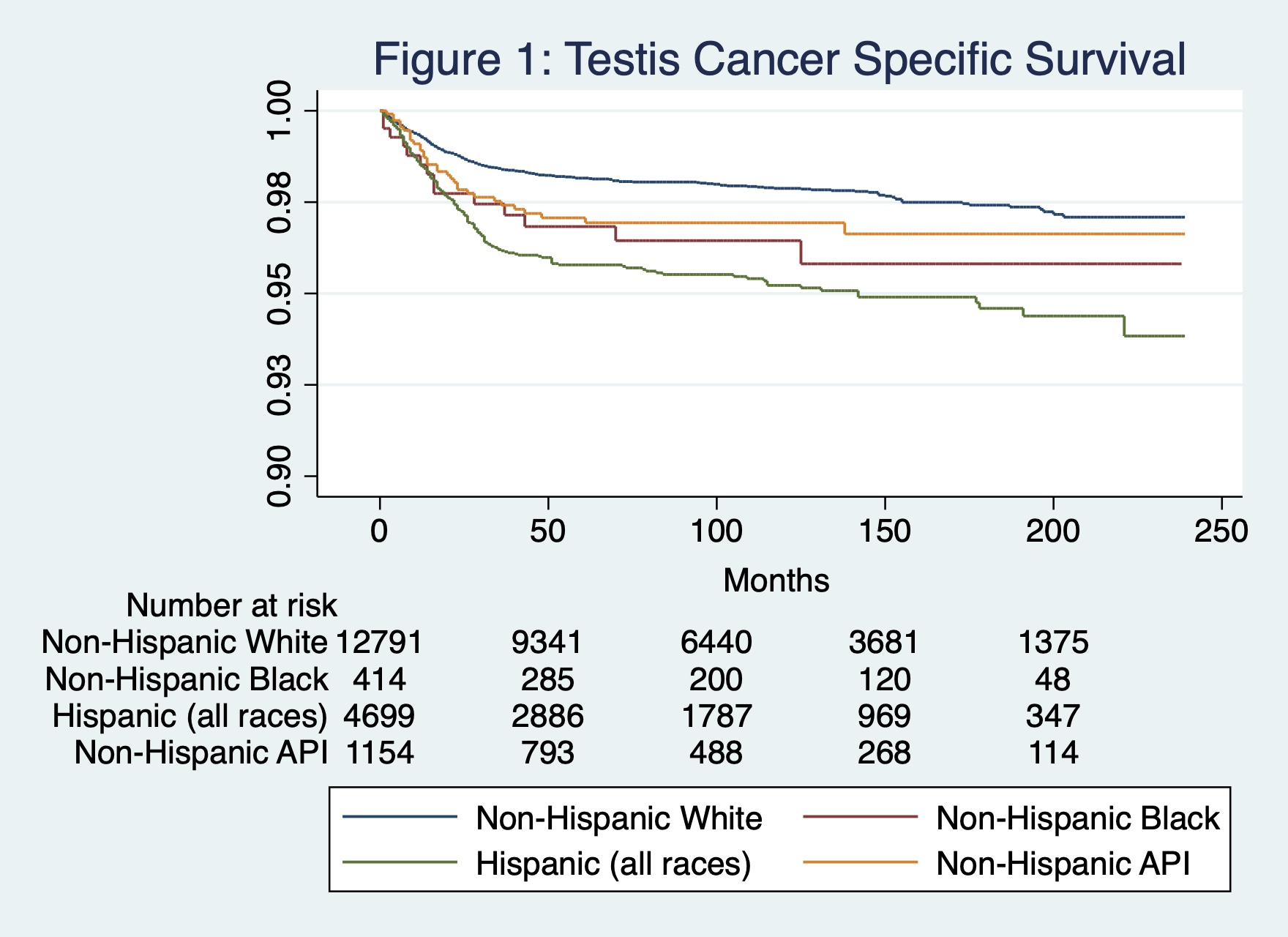
Introduction: The incidence of testis cancer among Hispanic men in the United States is increasing. Prior research has demonstrated that Hispanic patients exhibit a survival benefit for many medical conditions, a phenomenon known as the “Hispanic Paradox.” However, this paradox may not extend to testis cancer. We sought to examine survival outcomes in testis cancer by race using a large national sample. Methods: A population-based retrospective cohort study of testis cancer patients was performed using Surveillance, Epidemiology, and End Results (SEER) data for the years 2000 through 2019. Cox proportional hazards models were used to examine the relationship between race/ethnicity and testis cancer-specific survival, both overall and by histologic type (seminoma vs. nonseminomatous germ cell tumors [NSGCT]). All models were adjusted for age, stage, receipt of postoperative radiation or chemotherapy, year of diagnosis, income, marital status, and rural status. Results: The final analytic cohort consisted of 18,600 patients, of whom 66.8% were Non-Hispanic White (NHW), 2.2% Non-Hispanic Black (NHB), 24.9% Hispanic (all races), and 6.1% Non-Hispanic Asian or Pacific Islander (API). Median follow up was 92 months. Death from testis cancer occurred in 2.7% of patients. A greater proportion of Hispanics were diagnosed at an age less than 30 years (54.4%) and with initial metastatic disease (15.2%) compared to other groups. Hispanics experienced significantly worse cancer-specific survival (hazard ratio [HR] = 1.8, 95% CI: 1.5-2.2) compared to NHW patients overall (Figure 1). When stratified by tumor type, cancer-specific survival was significantly worse for Hispanics (HR = 1.8, 95% CI: 1.4-2.2) and API’s (HR = 1.6, 95% CI: 1.1-2.5) with NSGCTs. No difference was observed in cancer-specific survival by race/ethnicity for seminoma patients, however. Conclusions: Contrary to the Hispanic paradox reported across many medical conditions, cancer-specific survival is significantly worse for Hispanic men with testis cancer, particularly among those with NSGCT tumors. Future investigation of both public health and biological factors is needed to identify actionable drivers for this observed difference. SOURCE OF Funding: None