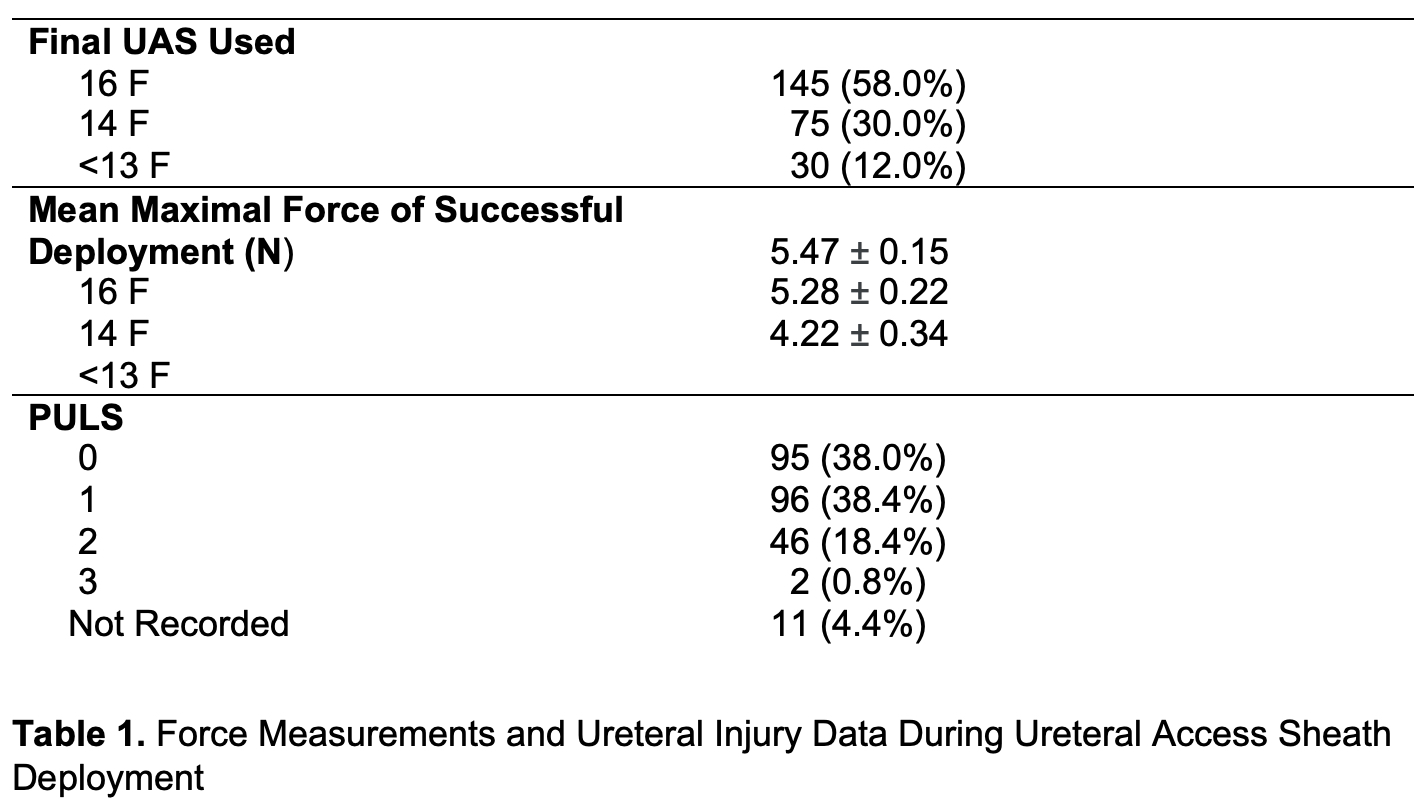
Introduction: During ureteroscopic stone therapy, the insertion of a 14 Fr ureteral access sheath (UAS) results in significant ureteral trauma in upwards of 20% of patients. In attempts to avert such injury, we developed a proprietary UAS force sensor. Our studies indicated that maintaining the force of insertion below 6 N would allow for non-injurious insertion of even a 16 Fr UAS. Herein, we sought to identify the clinical factors associated with the safe deployment of a 16 Fr UAS. Methods: Two hundred and thirty-eight patients (250 renal units) were subject to having UAS insertion forces recorded. In each case, an attempt was made to initially pass a 16 Fr UAS; if 6 N was reached, the surgeon was advised to downsize to a 14 Fr UAS and if 6 N was again reached, the surgeon was advised to downsize to a 12 Fr UAS. A post-ureteroscopic lesion scale (PULS) was recorded for each case to assess for ureteral injury. Regression models were created to estimate the impact of adjusted variables on PULS value, 16 Fr UAS deployment, and maximum UAS insertion force. Results: A 16 Fr UAS was deployed in 145 (58%) renal units with a mean maximum force of 5.5 N. Two renal units with high-grade ureteral injuries (PULS = 3) were noted; however, in both cases, the safety threshold (6 N) was exceeded: 8.36N and 8.91N. Preoperative stents were strongly associated with successful passage of a 16 Fr UAS independent of tamsulosin (OR 3.184, p = 0.002). Recently treated bacteriuria (OR 1.988, p = 0.033), and preoperative antibiotics (OR 1.96, p = 0.014) were also independent predictors of successful 16 Fr UAS deployment. Preoperative administration of tamsulosin was not found to be beneficial. Conclusions: Maintaining an insertion force of = 6 N can avoid significant UAS associated ureteral injuries. Preexisting indwelling stents, recently treated bacteriuria, and preoperative antibiotics favored safe insertion of a 16 Fr UAS. SOURCE OF Funding: None.