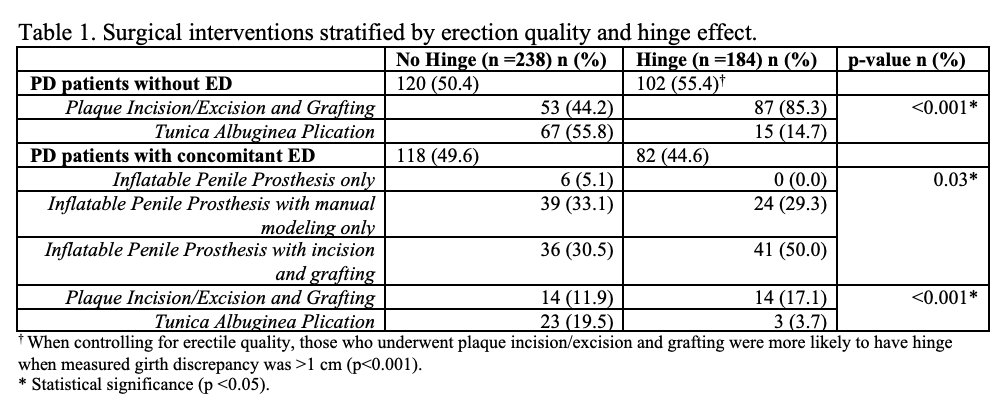
Introduction: Patients with Peyronie’s disease (PD) suffer from a variety of penile deformities including curvature, indentation, hourglass, shortening, and erectile dysfunction (ED). The presence of a hinge effect can be appreciated during penile duplex assessment (PDDU) as buckling or folding of the shaft when axial pressure is placed on the glans. Patients with hinge effect can experience bothersome buckling of the erection and instability during penetrative sex. The characteristics that cause hinge effect and its clinical implications are not fully understood. We aim to determine the PD factors that cause hinge effect and to assess the role of hinge effect on subsequent surgical intervention. Methods: Retrospective review was conducted on 1,483 patients presenting with PD from 2016-2021. Complete PDDU and hinge assessment were obtained in 1,223 included for analysis. Baseline demographics, PDDU findings, and clinical outcomes were obtained. Univariate and multivariate analyses were performed to assess for predictors of hinge effect. Results: Hinge effect was observed at the time of PDDU in 33% of PD patients. The degree of indentation (1.82 OR, p <0.001), rigidity of erections (0.82 OR, p=0.002), and degree of primary curvature (1.03 OR, p < 0.001) predicted presence of hinge effect. Furthermore, hinge effect greatly affected the type of surgical intervention required to correct PD deformity. Patients with hinge effect were more likely to require plaque incision/excision and grafting as opposed to tunica albuginea plication in PD patients with good quality erections. When controlling for erectile rigidity, patients who underwent partial plaque excision and grafting were more likely to have hinge when measured girth discrepancy was >1 cm (p < 0.001). In those requiring penile prosthesis, incision and grafting was more commonly required when hinge effect was present. Conclusions: The presence of hinge effect can be extremely bothersome and cause instability of erections during penetrative sex. Multiple factors may predispose to a hinge effect, including quality of erection and severity of curvature. When controlling for rigidity, a girth discrepancy of >1 cm did appear to pre-dispose to a hinge. Additionally, assessment of hinge effect pre-operatively was important in determining the optimal surgical intervention to correct PD deformities. SOURCE OF Funding: None

 photo")