UVA Urology Research Fellow The University of Virginia
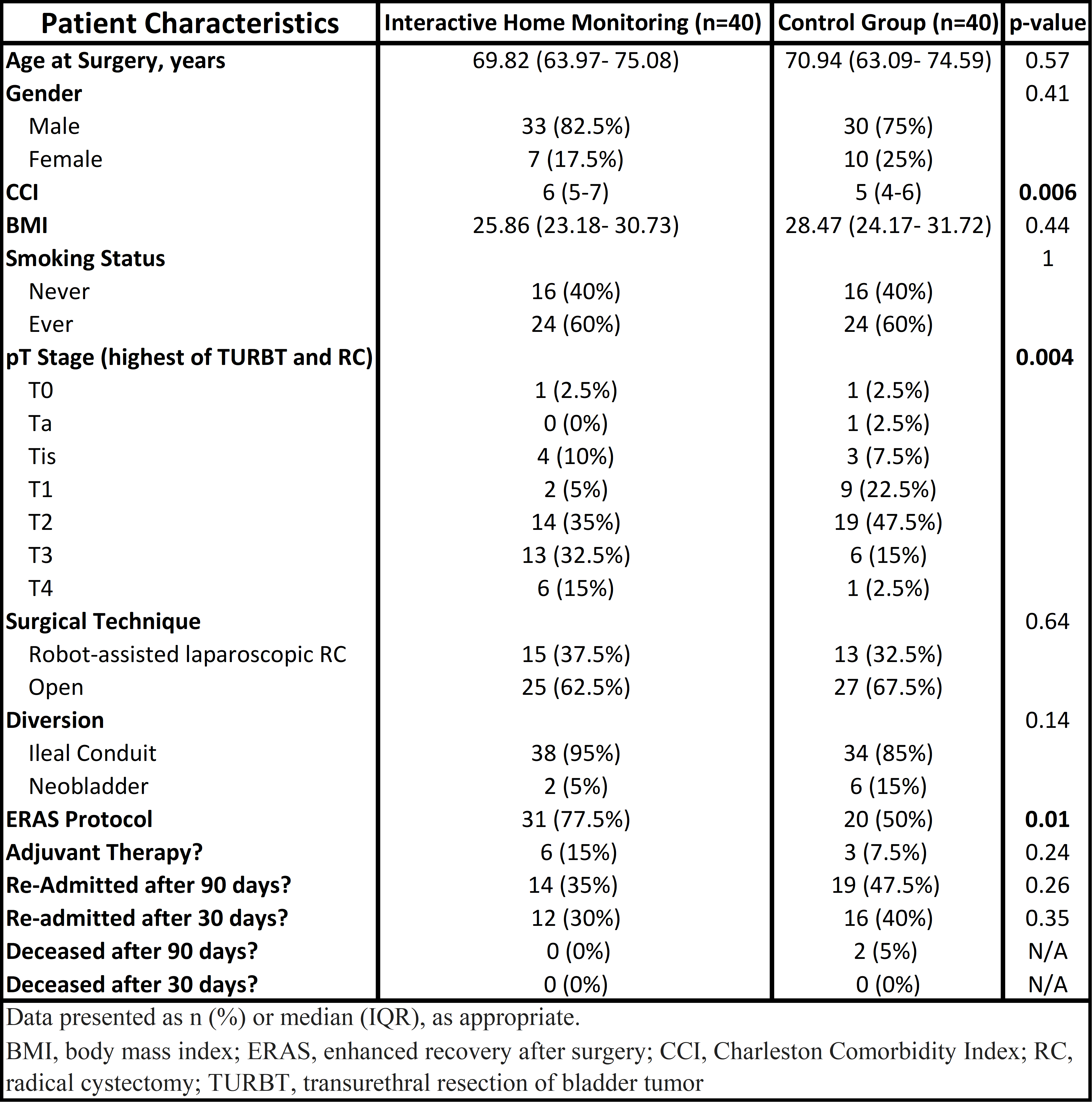
Introduction: Interactive home monitoring (IHM) is a comprehensive transition program designed to dynamically monitor and deliver post-surgical needs at home. This program not only assesses vitals and sends them directly into the electronic medical record but also combats barriers to healthcare and functions as an advocate for clinical follow-up. Use of IHM in radical cystectomy, a surgery with high risk of complications and re-admissions, has not been evaluated. This study assesses outcomes of radical cystectomy patients enrolled in IHM and compares results to a control group. Methods: Retrospective data was evaluated on all patients receiving radical cystectomy from September 2020 to June 2022. Primary outcomes are 90- and 30-day re-admissions and mortality. We defined cohorts based on IHM status and comparison tested was performed using chi-squared, Fisher’s exact, and student’s t-test. Multivariate linear regression was performed on combined cohorts to identify variables associated with outcomes. Results: A total of 80 patients were evaluated during the study period. Table 1 contains patient demographics. There were no differences in baseline characteristics between the IHM and control groups in age, gender, BMI, smoking status, surgical technique, diversion type, or adjuvant therapy. Charleston comorbidity index (p=0.006) and enhanced recovery after surgery protocol (ERAS) (p=0.011) differed between cohorts. When dichotomized by T2 or less vs greater than T2, the IHM group had higher cancer stage (p=0.004). The IHM group had 35% of patients with a 90 day re-admission and 30% with a 30 day re-admission. The control group had 47.5% of patients with a 90 day re-admission and 40% with a 30 day re-admission. Combination of cohorts showed ERAS to be a predictor of 90- (OR=0.10; P<0.001) and 30-day (OR=0.14; p<0.001) readmission on multivariate analysis. The IHM group had 0 (0%) deceased patients and the control group had 2 (5%) deceased patients 90 days following surgery. Conclusions: Although the IHM group had significantly more comorbidities and greater disease burden, the IHM group had a lower 35% 90-day readmissions relative to the control group’s 47.5% readmissions. This novel method of post-discharge continuity of care is appealing in the potential to discharge highly comorbid patients to their homes and decrease re-admission and mortality rates. SOURCE OF Funding: None.

 photo")