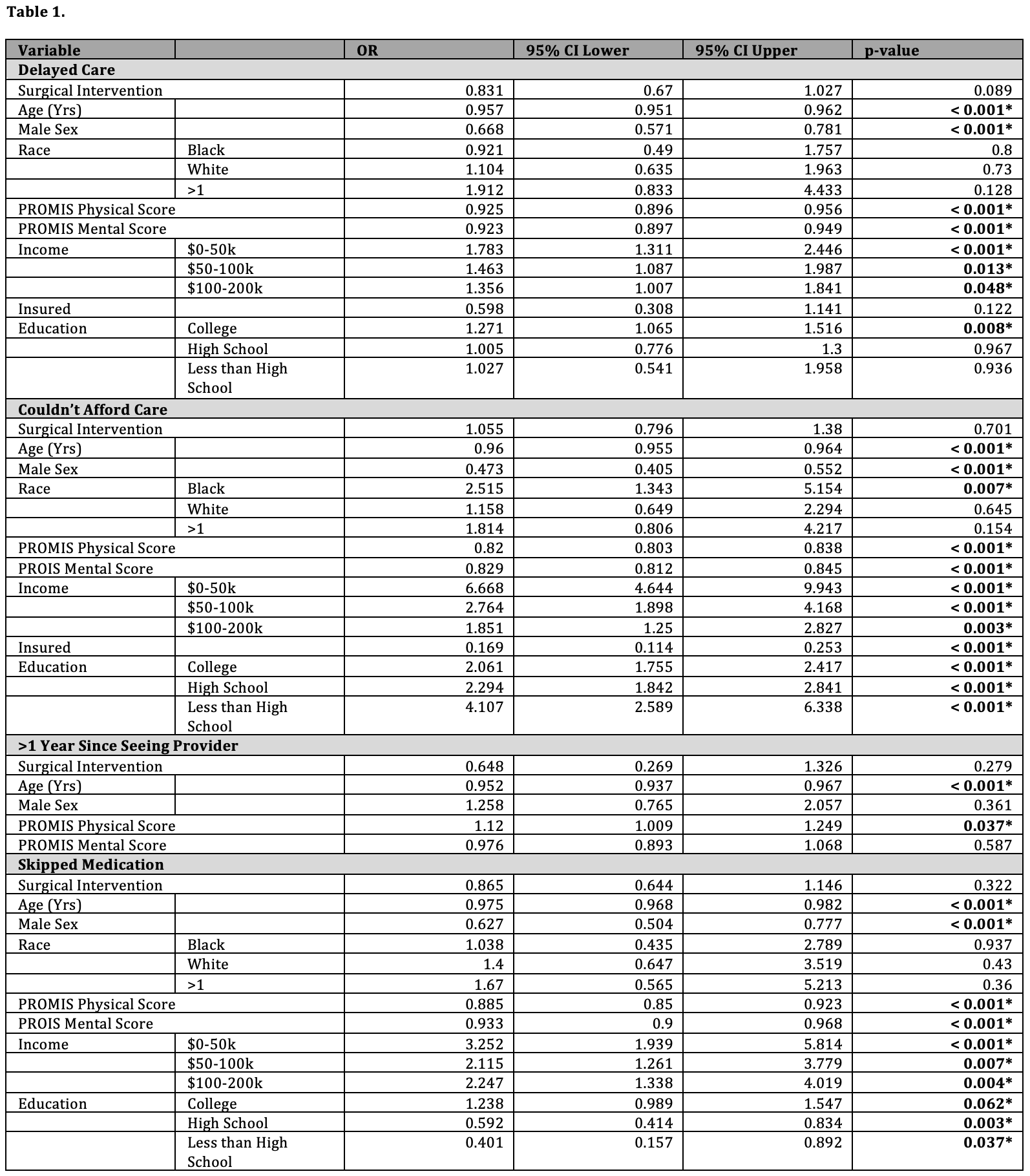
Introduction: Despite the high prevalence of kidney stones, little data exist regarding the prevalence of barriers to obtaining appropriate treatment. We sought to use a diverse dataset to evaluate and characterize the impact of nephrolithiasis diagnosis and treatment on healthcare utilization. Methods: We conducted a retrospective cohort study using the All of Us Database, an NIH database targeting recruitment of underrepresented US populations. Patients were included based on self-report of a diagnosis of kidney stones and were further categorized into surgical and non-surgical based on CPT codes. A control group without a diagnosis of nephrolithiasis was matched based on demographic and clinical characteristics. Primary outcomes were patients’ self-reported ability to access and afford care. Univariate and multivariable regression were performed. Results: In total, 9,173 patients with a diagnosis of nephrolithiasis were included and matched to controls. Compared to controls, patients with kidney stones were less likely to have had >1 year since last provider visit (1.7% vs. 3.8%, p<.001), but did not report increased delays obtaining care, inability to afford care, or skipping medications. Among patients with a stone diagnosis, 1,208 (13.2%) had been treated with surgical intervention (SWL, URS, PCNL). A delay in care was reported by 31% , 11.4% could not afford care, 12.9% skipped medications, and 1.7% had not seen a provider in >1 year. On multivariable analysis, prior surgical intervention was not associated with barriers to care. However, younger age, female sex, black race, lower income, lower education level, and lower physical health score were associated with delays obtaining care, inability to afford care, and skipping medications (Table 1). Conclusions: A diagnosis of kidney stones, subsequent intervention, and race were not associated with a significant increase in patient-reported barriers to care. However, among patients with nephrolithiasis, those of black race, younger, comorbid, female patients from lower socioeconomic status are at significant risk of being unable to access treatment. Further research to target specific groups and interventions will help better understand health discrepancies. SOURCE OF Funding: Mayo Clinic Department of Urology

 photo")