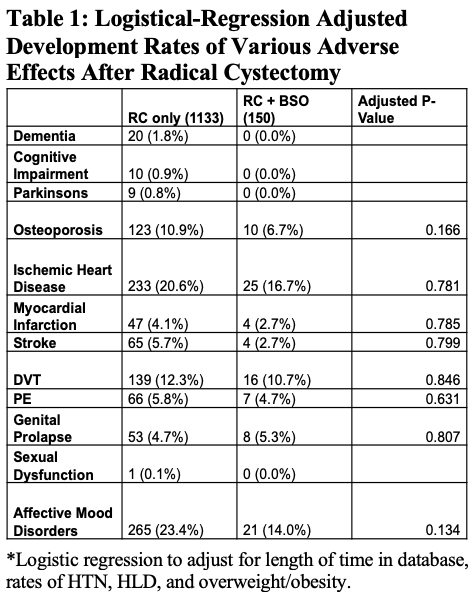
Introduction: AUA guidelines for radical cystectomy (RC) in women recommend removing adjacent reproductive organs including ovaries to reduce subsequent ovarian cancer (OC) risk. However, the most common histologic type of OC, high grade serous cancer, is now thought to originate from the fallopian tubes and many national level organizations now recommend bilateral salpingectomy (BS) for OC risk reduction at the time of abdominal surgery. Recent data also suggest that retention of post-menopausal ovaries is health beneficial. In the setting of ongoing debate regarding oophorectomy at the time of RC, rates of OC in a female population undergoing RC for bladder cancer need to be defined. Our objectives were: 1. To determine rates of OC in a female population undergoing RC for bladder cancer. 2.To determine rates of adverse effects associated with oophorectomy in this population. Methods: Retrospective cohort study conducted via TriNetX Research Network after IRB approval; final cohort contained 1,286 patients. Baseline demographic and clinical data were determined among patients undergoing RC and RC with concurrent bilateral salpingo-oophorectomy (BSO). Logistic regression analysis was used to evaluate associations between surgery performed and downstream co-morbid diseases. All statistical analysis conducted via Stata. Results: 1,133 patients underwent RC; 3 underwent RC and BS, and 150 underwent RC+BSO. At baseline, groups did not differ in age, race, ethnicity, or oncologic family or personal history; significant differences were noted in BMI, HTN, HLD, and overweight/obesity. Among those with RC, 1.3% developed OC and 0.5% developed peritoneal cancer. No significant differences were noted in development of adverse effects between the RC and RC+BSO groups (Table 1). No significant difference in all-cause mortality observed between RC and RC+BSO group (HR = 0.997 [0.827 – 1.203], log-rank p=0.979). Conclusions: Our study shows that 1.8% of females undergoing RC for bladder cancer develop ovarian or peritoneal cancer. This is consistent with the lifetime OC risk for the general population. Current performance of BS in lieu of BSO at RC is less than 1%. Whether BS can replace BSO for ovarian cancer risk reduction at the time of RC in patients with no known or suspected genetic risk for OC warrants further study. SOURCE OF Funding: NA

 photo")