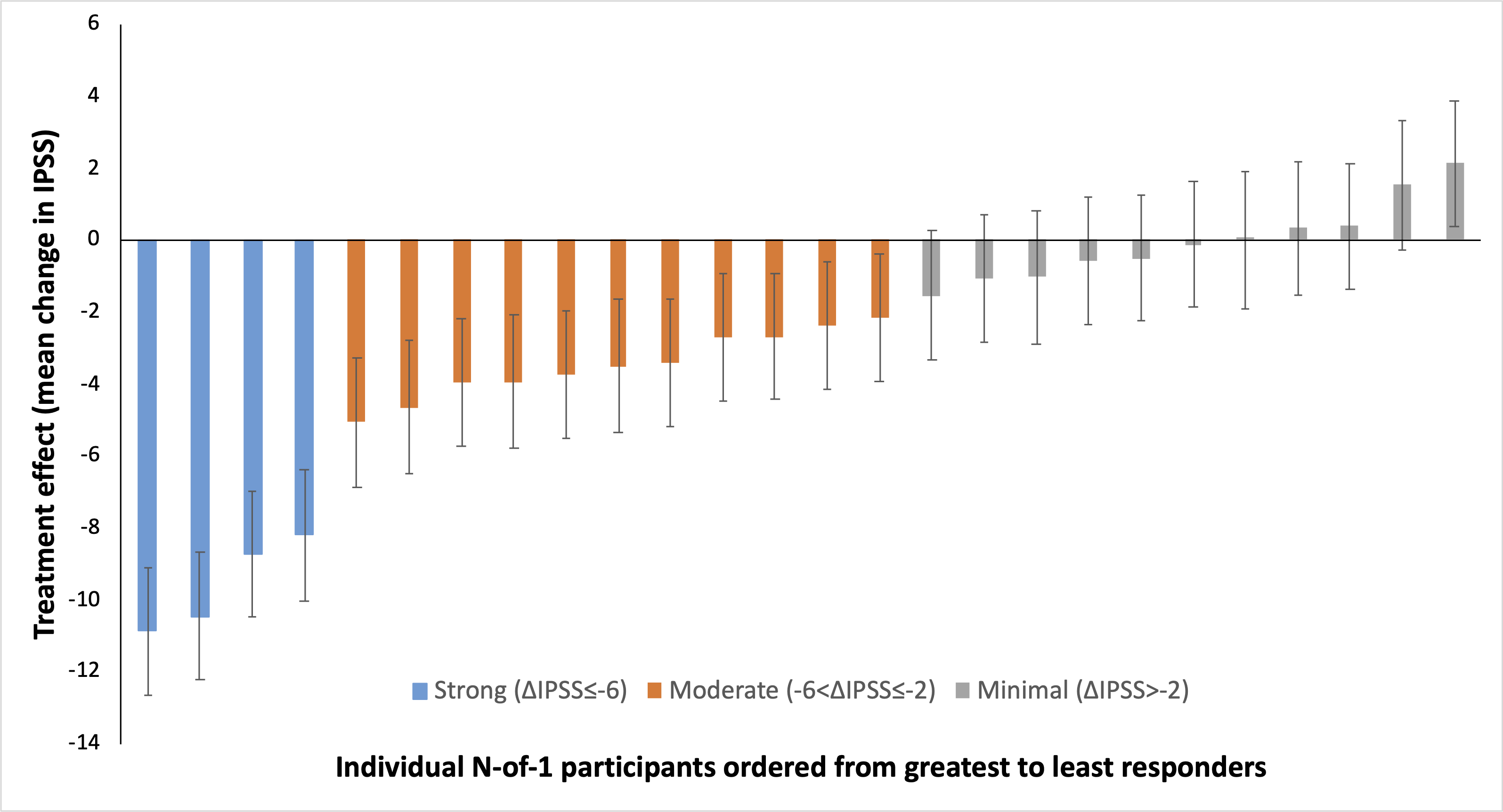
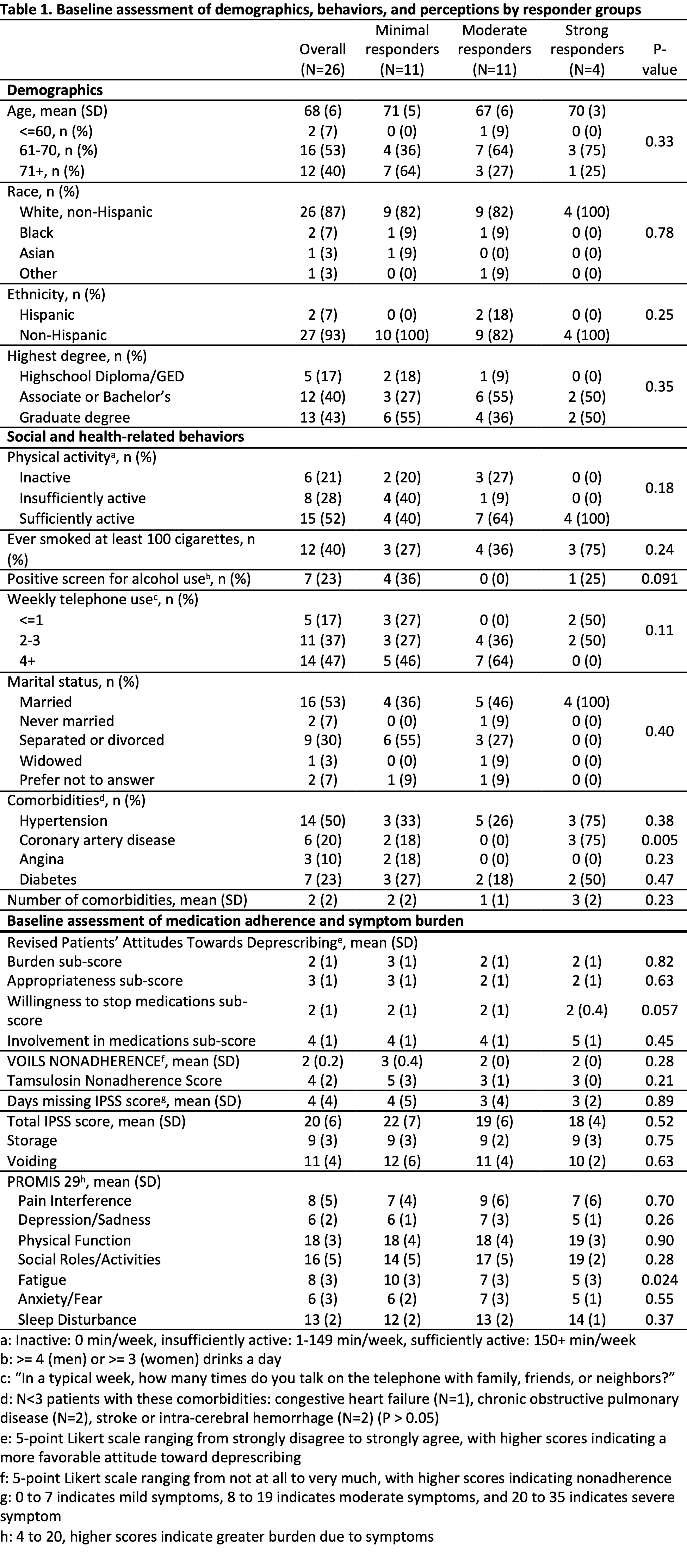
Introduction: Alpha blockers such as tamsulosin are considered 1st line for lower urinary tract symptoms (LUTS) due to benign prostatic hyperplasia (BPH). Despite widespread use, their efficacy versus placebo is modest/highly variable and adverse effects including orthostatic hypotension/falls in older men are costly. A personalized approach can identify patients in whom benefits outweigh harms and those who can be deprescribed without worsening LUTS or causing complications. Methods: We conducted placebo-controlled N-of-1 trials in men =55 on tamsulosin =12 months for BPH. To ensure tolerance of tamsulosin discontinuation, all men completed a one week run-in without taking tamsulosin or study pills. Participants then completed 2 block-randomized cycles, each comprised of two 2-week treatment periods of tamsulosin/placebo separated by 1 week of washout on placebo, and completed daily symptom assessment on REDCap (International Prostate Symptom Score (IPSS) modified for 24h recall). Linear mixed models adjusted for treatment period were used to calculate predicted random effects, representing the mean effect of tamsulosin for each participant. Results: 30/71 eligible patients contacted were enrolled. 4 failed run-in and were excluded. The remaining 26 were grouped by mean change in daily IPSS on tamsulosin vs. placebo and categorized as minimal (11/26, 42%), moderate (11/26, 42%), or strong responders (4/26, 15%) based on preset cutoffs (Figure 1). Demographics, social/health-related behaviors, and medical history except coronary artery disease (p = 0.005) were similar across groups (Table 1). Responder groups significantly differed in perceived fatigue from LUTS (p = 0.024) at baseline. Conclusions: It is feasible to conduct placebo-controlled N-of-1 trials in older men receiving tamsulosin using daily symptom reporting. Patients identified as minimal responders are candidates for deprescribing and alternative interventions. SOURCE OF Funding: UCSF-RAP

.jpg "Kevin Danis Li, BS (he/him/his) photo")