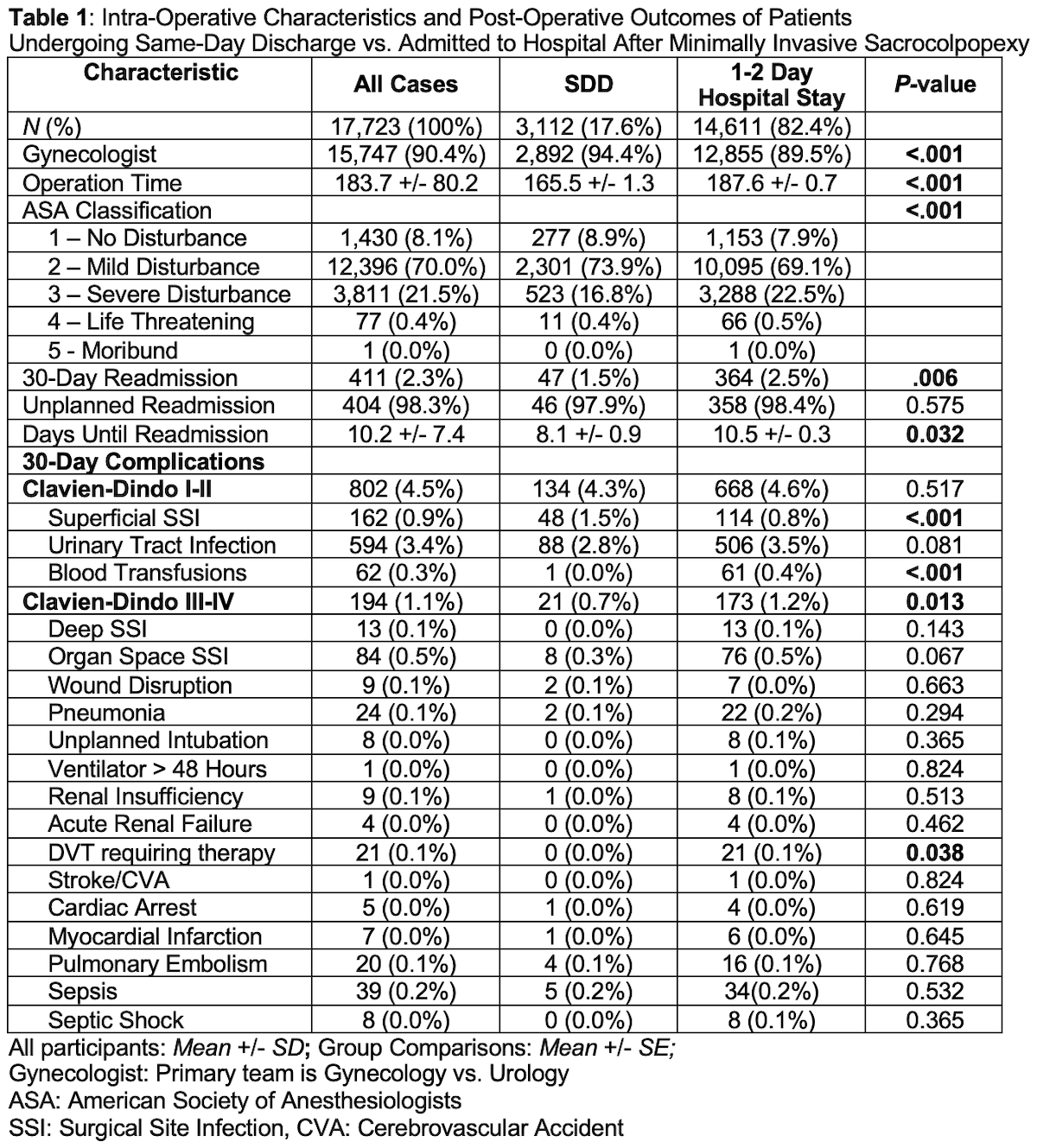
Introduction: Laparoscopic or robotic sacrocolpopexy (SCP) has become a preferred approach in women with pelvic organ prolapse. This study aims to evaluate trends and outcomes of same day discharge (SDD) laparoscopic or robotic SCP using the American College of Surgeons National Surgical Quality Improvement Program (NSPIQ) database. Methods: Patients were collected from the NSQIP database between 2012-2020 with the current procedural terminology code 57280. Patients with total hospital stay of 0 days were classified as SDD and compared to patients that were discharged on post-op day 1 or 2. The primary outcomes were 30-day complications and readmission rates. Demographic data and perioperative characteristics between the two groups were compared using the appropriate t-test, Chi-squared test, or Fisher’s exact test. Results: A total of 17,723 SCP were included. There were 3,112 (17.6%) same day discharges. There was a significant association between SDD SCP and year of operation (p <.001), with 31.0% of SCP in 2020 discharged on the same day in contrast to 10% of SCP in 2012. SDD patients were younger (56.8 vs. 58.9 years, p<.001), and had lower prevalence of diabetes (8.2% vs. 9.9%, p<.01) and hypertension requiring medications (30.9% vs. 36.9%, p<.001). SDD SCP were more frequently performed by gynecologists than urologists (94.4% vs. 89.5%, p<.001) and had lower operative time (165.5 vs. 187.6 minutes, p<.001). There were fewer cases of readmissions following SDD (1.5% vs. 2.5%, p<.01). Post-operatively, SDD cases were associated with more superficial surgical site infections (1.5% vs. 0.8%, p<.001), but significantly fewer cases of class III-IV complications (0.7% vs. 1.2%, p<.05, Table 1). Conclusions: There has been a steady rise in SDD after minimally invasive SCP with no significant association of increased risk for serious complications. With further patient education on wound care, SDD after minimally invasive SCP may be a safe and less costly alternative in the surgical management of pelvic organ prolapse. SOURCE OF Funding: None.