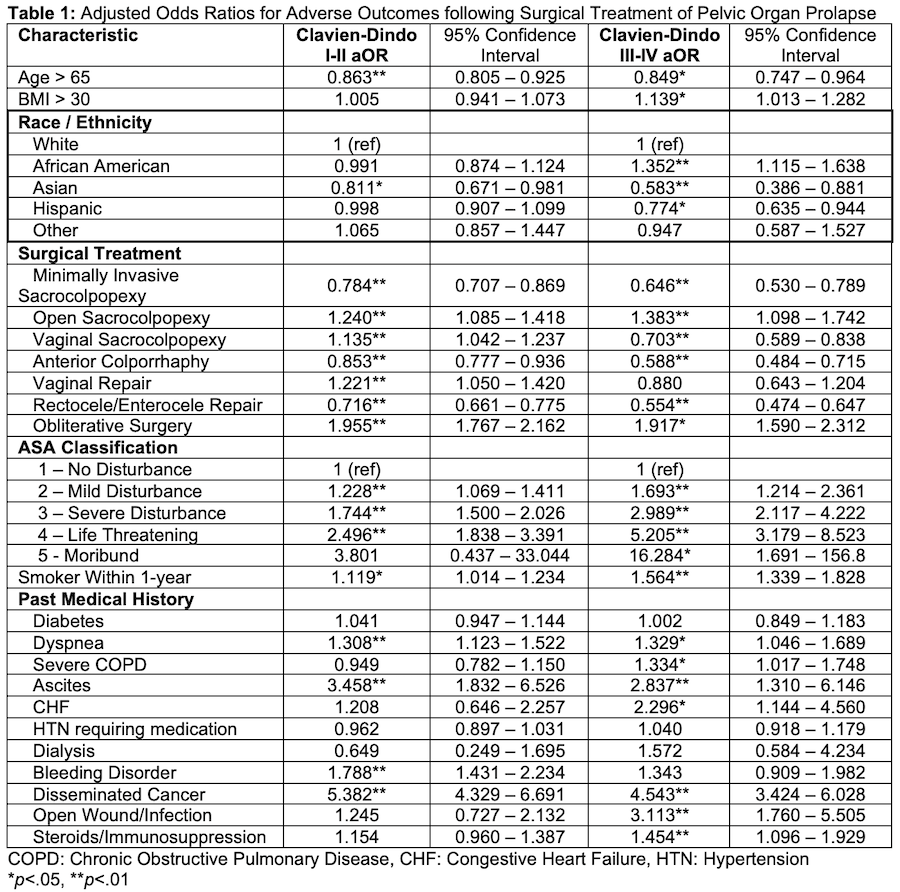
Introduction: Pelvic organ prolapse (POP) is a common condition with a 12.5% risk of surgical treatment by age 80. Prior studies have shown racial differences in outcomes of surgical treatment of POP in the US. Our study investigates whether there are racial disparities in adverse outcomes following surgical treatment of POP in the American College of Surgeons National Surgical Quality Improvement Program (NSPIQ) database. Methods: Patients were collected from the NSPIQ database between 2011-2020 with current procedural terminology codes for minimally invasive and open sacrocolpopexy, vaginal vault suspension, anterior colporrhaphy, vaginal repair, enterocele/rectocele repair, and obliterative surgery. Reported complications were aggregated into composite Clavien-Dindo I-II and III-IV classifications. Multivariate logistic regression was utilized to calculate adjusted odds ratios (aOR) for complications. Age, BMI, past medical history, smoking history, surgical treatment, and ASA score were included as covariates in the regression model. Results: Within Clavien Dindo III-IV complications, African Americans had a 35% increased risk (aOR: 1.35, p<.01), while Asians and Hispanics had a 42% (aOR: 0.58, p<.01) and 23% (aOR: 0.77, p<.01) decreased risk, respectively. Asian race was associated with a 19% decreased risk of Clavien-Dindo I-II complications (aOR: 0.81, p<.05) compared to White patients, with all other ethnicities bearing similar risk. Age >65 was associated with a 14% decreased risk of Clavien-Dindo I-II complications (aOR: 0.86, p<.01) and 15% decreased risk of Clavien-Dindo III-IV complications (aOR: 0.85, p<.01). Comorbidities of dyspnea, severe COPD, ascites, CHF, disseminated cancer, open wound/infection, steroids/immunosuppression, smoking history, and BMI >30 were significantly associated with higher odds of Clavien-Dindo III-IV complications (p <.05) (Table 1). Conclusions: African American women receiving surgical treatment for POP have increased risk of high-grade complications even when adjusted for age, past medical history, smoking status, and type of surgery. Further research is needed to elucidate implicit biases or disparities in healthcare that may contribute to adverse outcomes. SOURCE OF Funding: None.