MP08-02: Risk score-based substratification improves surveillance costs after transurethral resection of bladder tumor in patients with high-risk non-muscle-invasive bladder cancer
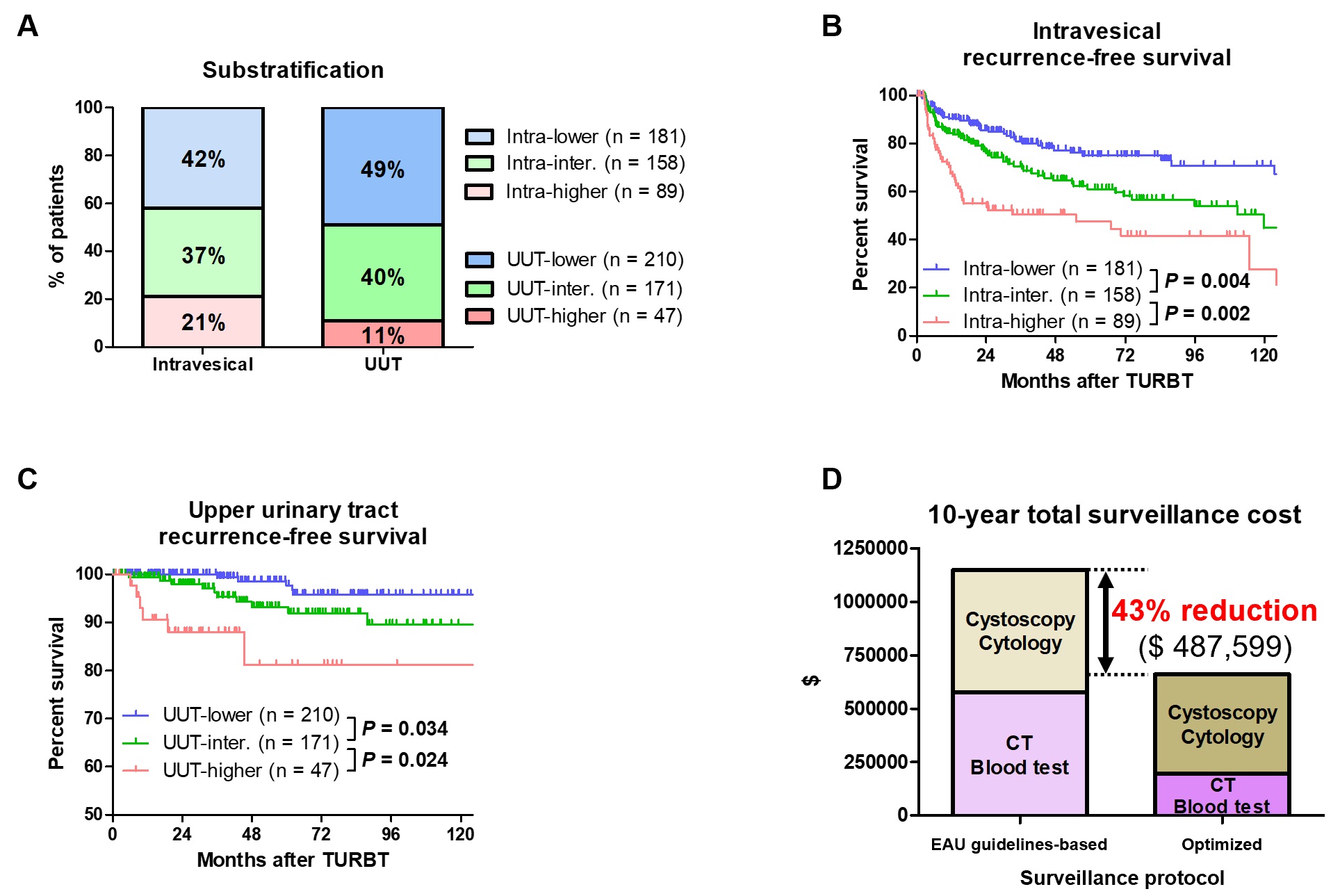
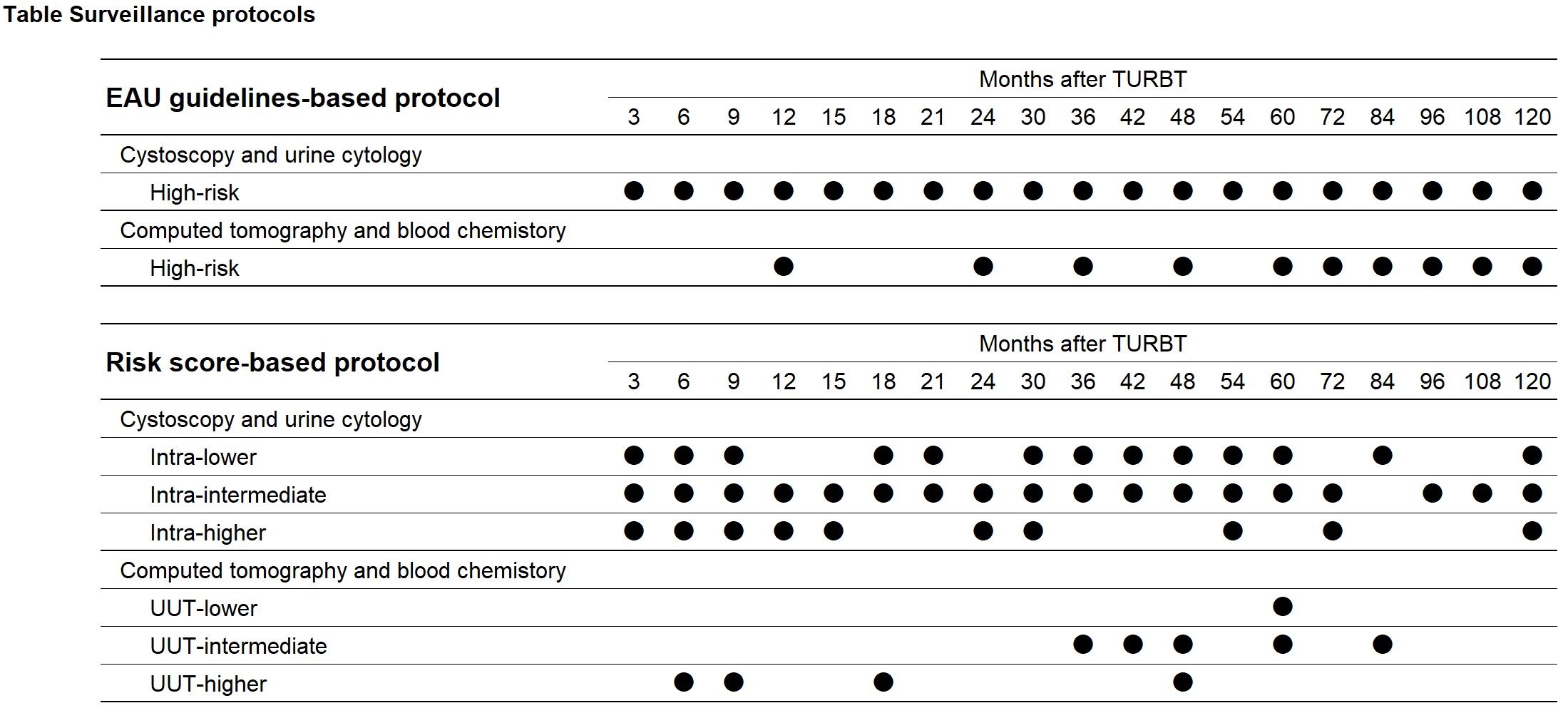
Introduction: The aim of the present study was to develop optimized surveillance protocols based on the risk score-based substratifications to improve surveillance costs. Methods: We retrospectively evaluated 428 patients with high-risk NMIBC who underwent TURBT from November 1993 to April 2019. Independent risk factors for intravesical and upper urinary tract (UUT) recurrences were assessed by multivariable analyses. Patients were substratified into intra-lower, intra-intermediate, and intra-higher groups or UUT-lower, UUT-intermediate, and UUT-higher groups by summing each of the independent risk factors of intravesical and UUT recurrences, respectively. Optimized surveillance protocols to enhance cost-effectiveness were developed using real incidences of recurrence after TURBT. The 10-year total surveillance costs were compared between the European Association of Urology (EAU) guidelines-based and optimized surveillance protocols. Results: Median age and follow-up periods were 72 years and 54 months, respectively. Multivariable analyses showed that chronic kidney disease, tumor size =30 mm, and grade 3 were independently associated with intravesical and/or UUT recurrences. Patients were substratified into intra-lower (0 score), intra-intermediate (1 score), and intra-higher (2 or 3 scores) groups for the intravesical recurrence risk estimation or into UUT-lower (0 score), UUT-intermediate (1 score), and UUT-higher (2 scores) groups for the UUT recurrence risk estimation (Fig. A). The Kaplan–Meier curves of intravesical and UUT RFS could be clearly separated among the three groups (Fig. B and C). Optimized surveillance protocols (Table) promoted a 43% reduction in the 10-year total surveillance cost compared with the EAU guidelines-based surveillance protocol (Fig. D). Conclusions: Optimized surveillance protocols based on risk score-based substratifications could potentially improve surveillance costs after TURBT in patients with high-risk NMIBC. SOURCE OF Funding: none