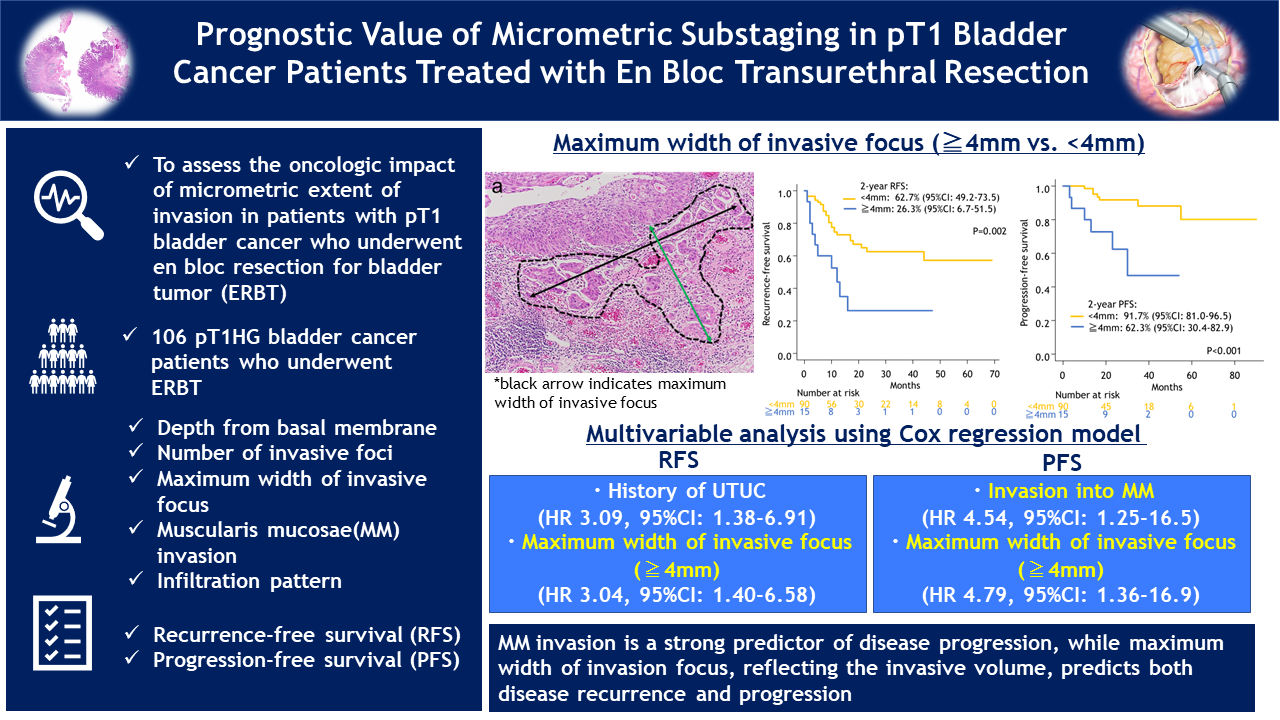
Introduction: We aimed to assess the oncologic impact of micrometric extent of invasion in patients with pT1 bladder cancer who underwent en bloc resection for bladder tumor (ERBT). Methods: We retrospectively analyzed the records and specimens of 106 pT1 high-grade bladder cancer patients who underwent ERBT at multiple institutions. The extent of invasion such as depth from basal membrane, number of invasive foci, maximum width of invasive focus, muscularis mucosae invasion, and infiltration pattern were evaluated by a single genitourinary pathologist. For classification of infiltration pattern, we defined solid sheet-like, nodular or nested growth pattern as pattern A, and trabecular, small cluster or single cell pattern as pattern B. The endpoints were recurrence-free (RFS) and progression-free survival (PFS) stratified by invasion degrees. Results: Overall, 24 patients (23%) had depth from basal membrane?1.3mm, 15 patients (14%) had maximum width of invasive focus?4mm, 32 patients (30%) had invasion into or beyond muscularis mucosae (MM), and 85 patients (80%) had infiltration pattern B. Within a median follow-up of 23 months, overall, 36 patients experienced disease recurrence and 13 patients experienced disease progression. The 2-year PFS significantly differed depending on depth from basal membrane ( <1.3mm: 94.8% vs. ?1.3mm: 65.2%, p=0.005), maximum width of invasive focus ( <4mm: 91.7% vs. ?4mm: 62.3%, p<0.001), MM invasion (above MM: 96.1% vs. into or beyond MM: 64.8%, p=0.002), and infiltration pattern (pattern A: 100% vs. pattern B: 83.3%, p=0.037). In a multivariable analysis that adjusted for the effects of standard predictors, MM invasion was an independent prognostic factor of progression (hazard ratio [HR]: 4.54, 95% confidence interval [CI]: 1.25-16.5). The maximum width of invasive focus?4mm was an independent prognostic factor of both recurrence (HR: 3.04, 95%CI: 1.40-6.58) and progression (HR: 4.79, 95%CI: 1.25-16.5). Conclusions: For T1 high-grade bladder cancer, MM invasion is a strong predictor of disease progression, while maximum width of invasion focus, reflecting the invasive volume, predicts both disease recurrence and progression. These two pathologic features could be used to further risk-stratify the heterogenous group of T1 bladder cancers. SOURCE OF Funding: None.