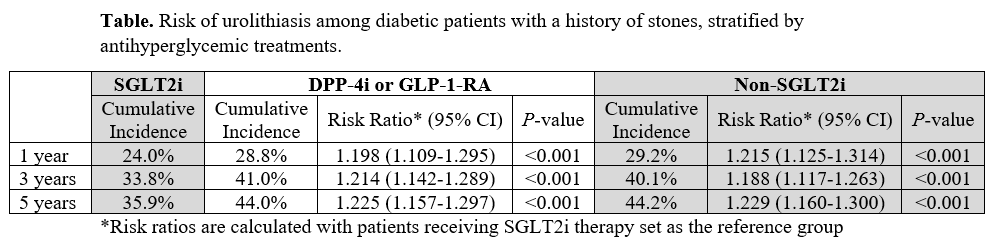
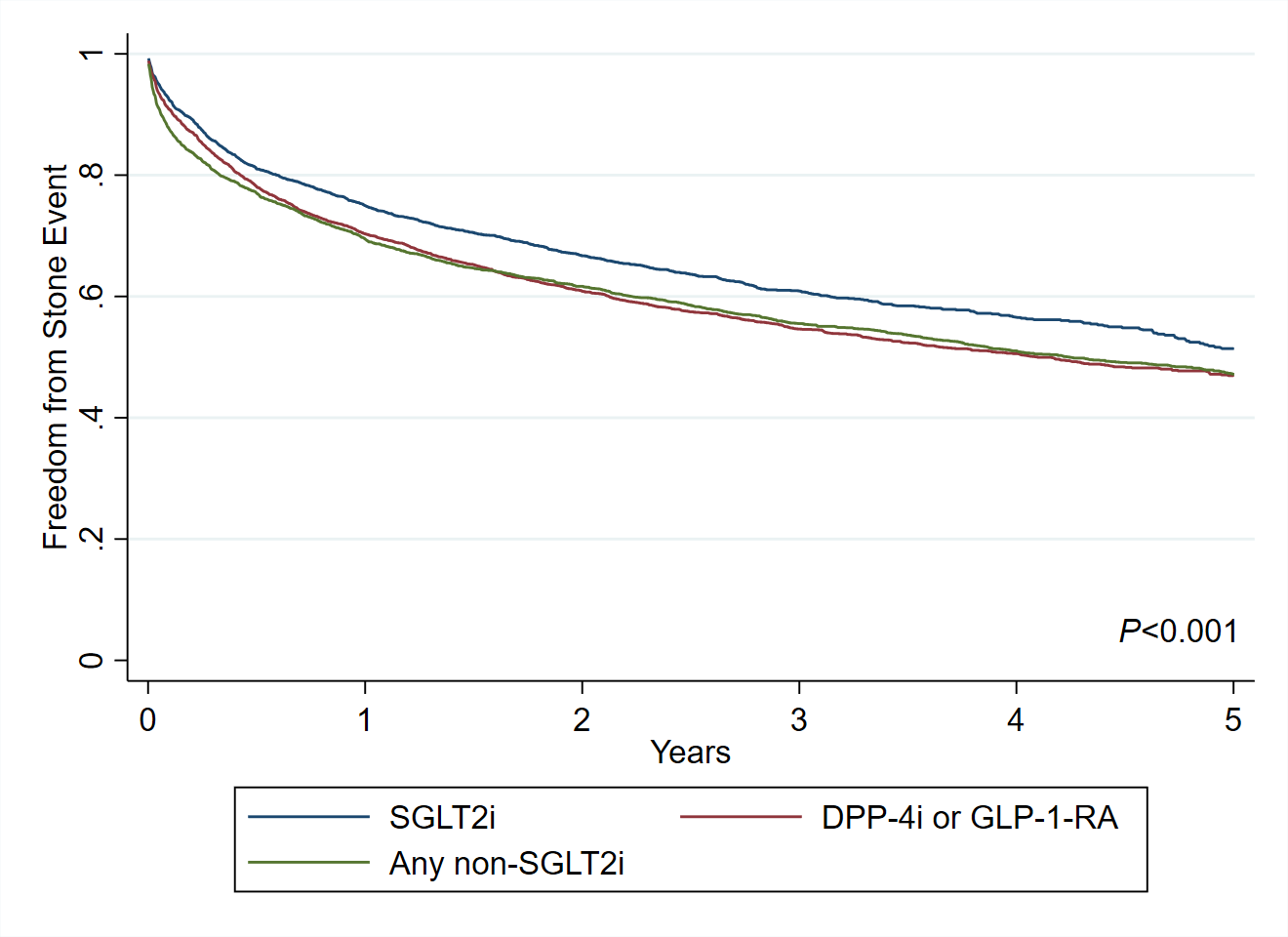
Introduction: Sodium-glucose cotransporter 2 inhibitors (SGLT2i) have emerged as a treatment for diabetes mellitus with additional cardiovascular and renal benefits over other classes of antihyperglycemics. Promising data suggests that SGLT2i may also reduce the risk of urolithiasis. We compared the risk of urolithiasis among diabetic patients with a history of stones prescribed SGLT2i versus other antihyperglycemics. Methods: TriNetX is a collaborative research enterprise with real-time data from over 70 healthcare organizations with more than 100 million patients. We queried the database for adult patients presenting between 1/1/2016 and 1/1/2021 with type 2 diabetes mellitus and a prior history of urolithiasis. Patients receiving SGLT2i therapy were compared against two groups: (1) patients receiving dipeptidyl peptidase 4 (DPP-4i) or glucagon-like peptide-1 receptor agonist (GLP-1-RA) and (2) all patients not receiving SGLT2i. Propensity score matching was performed to control for confounding. The risk of urolithiasis was compared at 1, 3, and 5 years after initiation of therapy, and Kaplan-Meier analysis was used to determine freedom from a stone event. Results: Among diabetics with a history of stones, SGLT2i was prescribed to 3,576 patients, DPP-4i or GLP-1-RA to 17,952 patients, and any non-SGLT2i to 131,592 patients. After matching, each group contained 3,572 patients. The cumulative incidence of urolithiasis in patients prescribed SGLT2i was 24.0% at 1 year, 33.8% at 3 years, and 35.9% at 5 years. In comparison, the risk of urolithiasis was approximately 20% higher at each timepoint when patients were prescribed DPP-4i or GLP-1-RA, or any non-SGLT2i therapy [Table]. As such, patients taking SGLT2i demonstrated the highest rates of freedom from a stone event over the course of 5 years (P <0.001) [Figure]. Conclusions: When managing diabetic patients with a history of stones, the use of SGLT2i presents an attractive option due to the significantly decreased risk of future stone events when compared to other antihyperglycemic medications. SOURCE OF Funding: None.