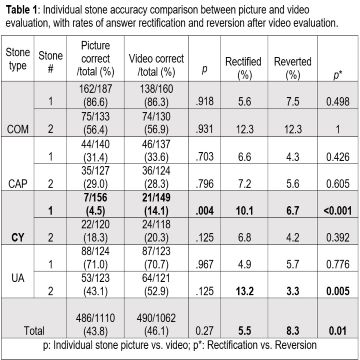
Introduction: Kidney stone analysis to determine composition is important for metabolic management and recurrence prevention. This analysis may be limited with dusting techniques, and many practices require lab outsourcing or additional resources, ultimately increasing healthcare costs. Studies have shown that Urologists have poor accuracy when attempting to identify stone types using simple visualization. We hypothesized that Urologists would more accurately identify stone types using video clips of stone dusting during laser lithotripsy compared to still pictures. Methods: We obtained representative pictures and videos during 8 ureteroscopies with holmium laser dusting of 4 stone types: calcium oxalate monohydrate (COM), calcium phosphate (CAP), cystine (CY) and uric acid (UA). Laser settings were 0.4 J x 50Hz across all cases. A Redcap survey was created and sent via email to the members of the Endourological Society. The survey included a picture followed by the corresponding video of each stone being dusted along with Hounsfield units (HU), size and location. Each picture and video included multiple-choice questions about stone composition and confidence level, ranging from 1 (very unsure) to 5 (very confident). Accuracy, confidence levels, and rates of rectification (change from incorrect to correct answer) or reversions (correct to incorrect) after watching videos were analyzed. Results: 187 trained urologists responded to the survey. The accuracy rate of pictures alone was 43.8 % vs. 46.1 % with videos (p = 0.27). Correct identification of individual stones was low, with high variability within stone types (Table 1). Video only improved accuracy for one CY stone. Confident answers (level 4 or 5) were more likely with videos than pictures (65.4% vs. 53.7%, respectively; p <0.001). Confident responses were also more likely to be correct than incorrect (66.1% vs. 53.9%, p <0.001). After viewing videos, participants were more likely to rectify their answers, with UA and CY stones having a higher proportion of rectified vs. reverted responses. Conclusions: Stone identification accuracy is low irrespective of confidence level, picture and video stone visualization, or knowledge of HU. Urologists should be cautious in using endoscopic stone appearance to direct metabolic management. SOURCE OF Funding: None