Session: MP11: Prostate Cancer: Advanced (including Drug Therapy) I
MP11-12: Development of a risk model for time to second progression in patients with high-risk metastatic castration-sensitive prostate cancer treated with abiraterone acetate and androgen deprivation therapy
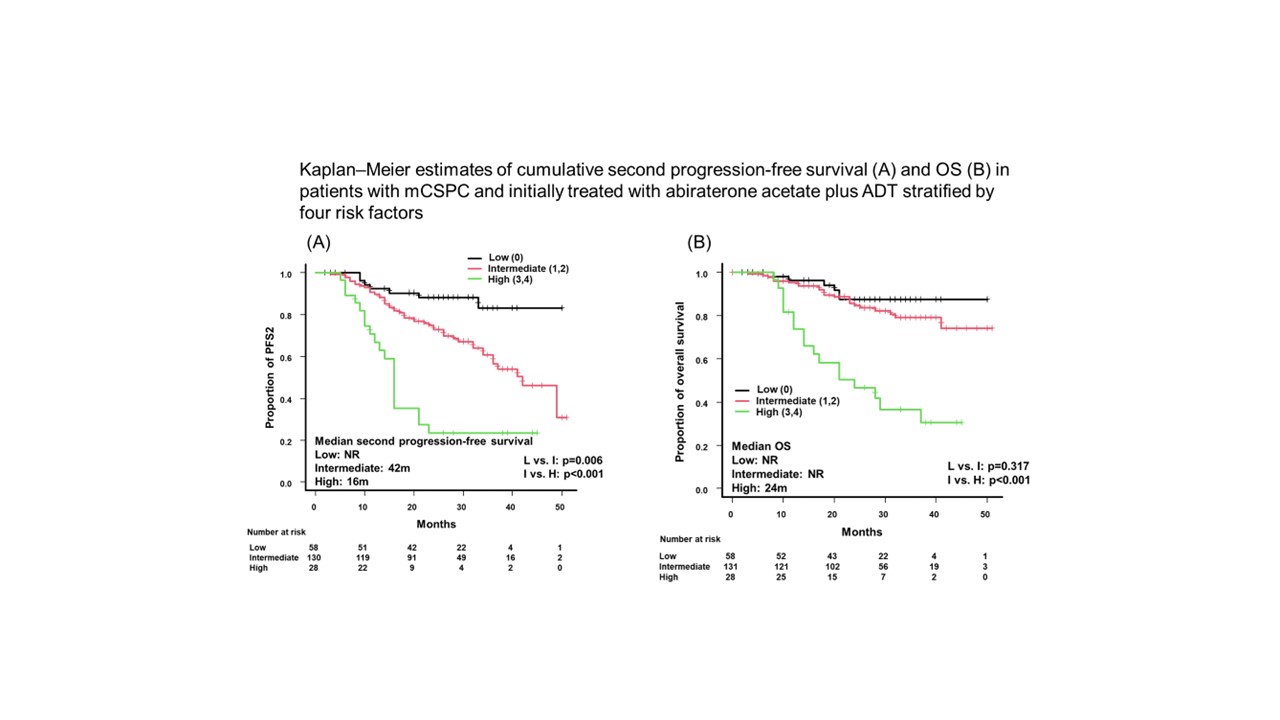
Introduction: Evidence on risk stratification in patients treated with doublet therapy with abiraterone acetate is limited. In this study, we developed a risk stratification model in patients with de novo high-risk mCSPC who received abiraterone acetate plus androgen deprivation therapy based on clinical risk factors. Methods: Medical records of 224 high-risk patients with de novo mCSPC treated with abiraterone acetate plus androgen deprivation therapy at 11 centers between 2015 and 2022 were retrospectively reviewed. Castration-resistant prostate cancer (CRPC)-free, progression-free survival 2 (PFS2), and overall survival (OS) were estimated using the Kaplan–Meier method. The association of pretreatment clinical risk factors with PFS2 was evaluated by Cox proportional hazard models and survival outcomes were classified according to the number of risk factors. Results: Median PFS2 was 43 months; second-progression occurred in 76 (34.2%) patients. On multivariable analysis, the following four risk factors were identified as independent predictors of PFS2: primary Gleason pattern 5 (HR 1.97, 95% CI 1.20–3.22), presence of liver metastasis (HR 2.05, 95% CI 1.02–4.13), extent of disease score = 3 (HR 2.25, 95% CI 1.16–4.34), and abnormal hemoglobin (HR 1.73, 95% CI 1.02–2.92). Significant differences in PFS2 were observed among the three risk groups (low vs. intermediate; p = 0.006, intermediate vs. high; p < 0.001). Median PFS2 and OS of high-risk patients were significantly worse in the low- and intermediate-risk groups. The median PFS2 of low-risk patients with no or one factor was not reached, whereas that of intermediate-risk patients with two or three factors and high-risk patients with four factors were 42 months and 16 months, respectively. Median OS was 24 months in high-risk patients, whereas it was not reached in low- and intermediate-risk patients. Conclusions: We successfully classified patients with high-risk mCSPC treated with abiraterone acetate based on four clinical risk factors. Risk-adapted treatment may be beneficial for selected patients with mCSPC in this triplet therapy era. SOURCE OF Funding: none