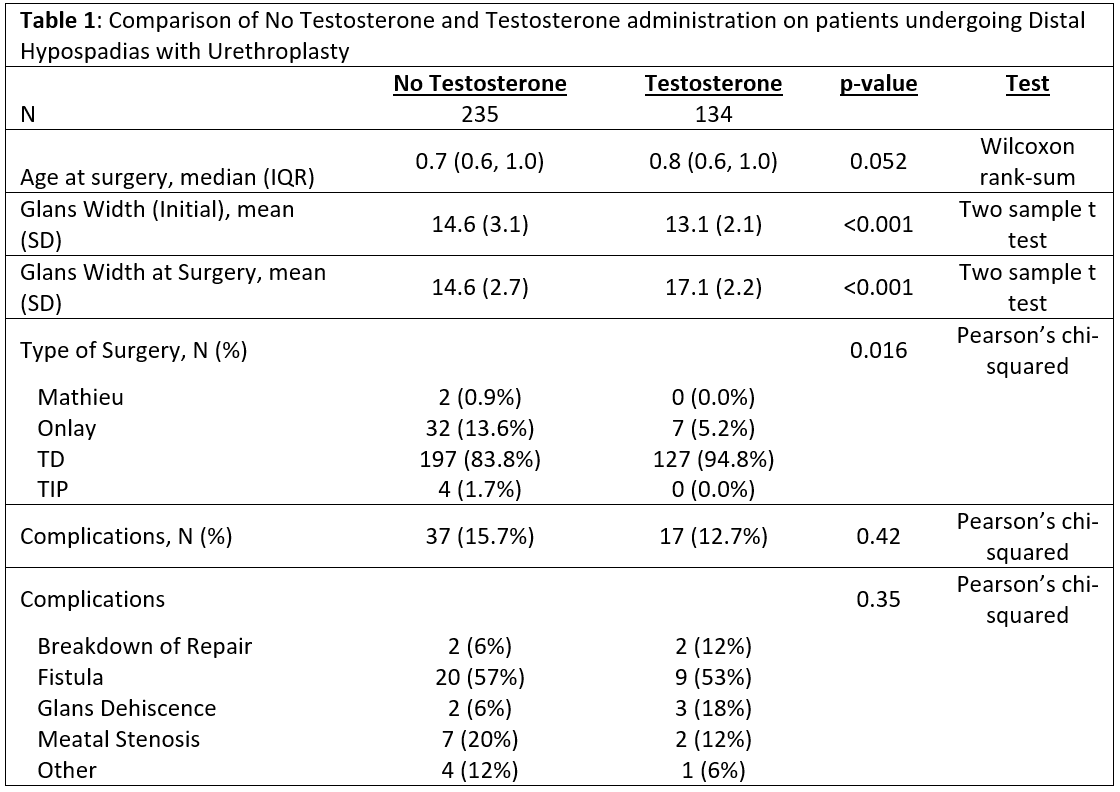
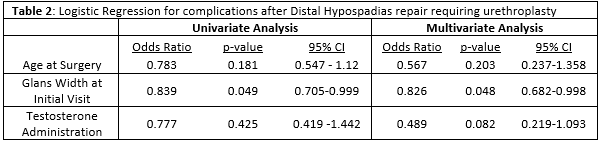
Introduction: Testosterone (T) administration prior to hypospadias repair is common practice among pediatric urologists, however its impact on surgical outcomes remains controversial. We hypothesize that T administration prior to distal hypospadias repair with urethroplasty significantly decreases postoperative complications. Methods: We queried our hypospadias database for primary distal hypospadias repairs with urethroplasty from 2016-2021. Patients undergoing repair without urethroplasty (MAGPI, MIV, urethral advancement) were excluded. We collected information on patient age, procedure type, T administration status, initial visit and intraoperative glans width (GW), and postoperative complications. To determine the role of T administration on incidence of complications a logistic regression adjusting for initial visit GW and age was performed. Results: Of 543 total patients with distal hypospadias in our database, 369 underwent hypospadias repair with urethroplasty. 134 patients received T, 235 did not. Median age was similar between groups (0.7 vs 0.8 years; p>0.05). Initial visit GW was significantly larger in the no T vs. T group (14.6mm vs 13.1mm). T patients had significantly larger glans width at the time of surgery (17.1mm vs 14.6 mm; p<0.05)). On univariate analysis no significant difference in complications was found between the T and no T groups, 12.7% vs 15.7% respectively, (p=0.42). Multivariate analysis showed T administration was not associated with a significant decrease in complications (OR 0.48; 0.2-1.09; p=0.08), but larger glans width at initial visit was (OR 0.83, p=0.048). Conclusions: In our cohort of patients undergoing distal hypospadias repair with urethroplasty preoperative T administration did not significantly decrease postoperative complications although there was a strong trend towards significance on multivariable analysis. A multi-institutional effort with a larger cohort may be necessary to show significance in response to T and to externally validate these findings. SOURCE OF Funding: -