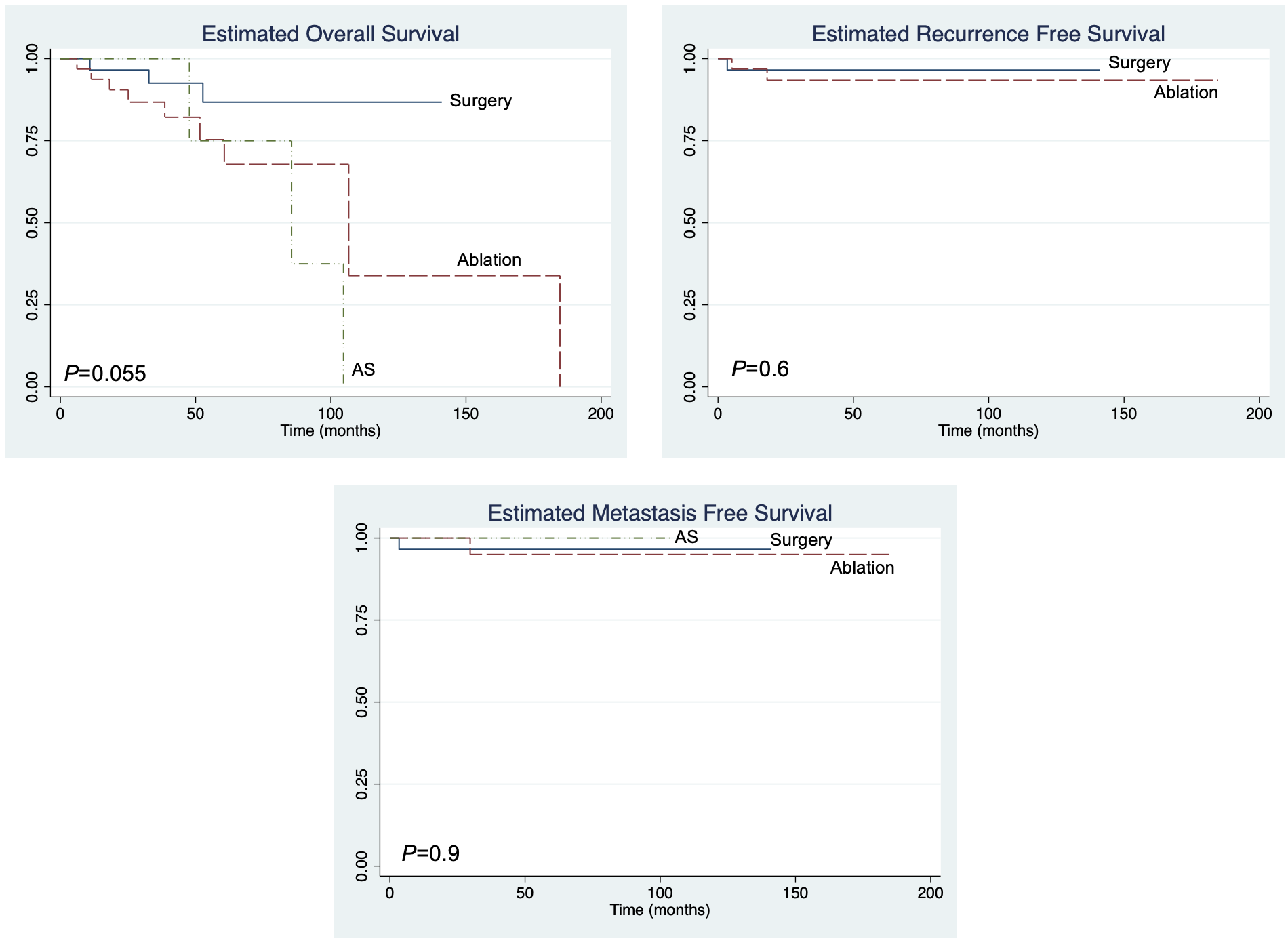
Introduction: Although there is a paucity of data, non-metastatic small renal cell carcinoma (RCC) patients who are medically immunosuppressed because of a prior organ transplant or treatment of an underlying disease have a theoretically higher risk of disease progression. This study describes the treatment and outcomes of medically immunosuppressed patients with clinical T1 RCC (cT1). Methods: An institutional database of patients treated or biopsied for RCC was queried for patients with pathologic diagnosis of cT1 RCC and were on chronic medical immunosuppression, defined as use of a WHO designated immunosuppressant or prednisone =5mg for at least 3 months prior to treatment of RCC and continued use during follow up. Outcomes for patients undergoing 1) surgery 2) ablation or 3) active surveillance (AS) are described. Wilcoxon Rank Sum, Fisher’s exact test and Kaplan Meier analysis was performed. Results: Between 2010-2022, 74 medically immunosuppressed patients with RCC were identified who were treated with surgery (n=29), ablation (n=33), or AS (n=12). Median age was 60 years (IQR 51-68), median Charlson comorbidity index was 3 [IQR 2-5] and median follow-up was 48 months (IQR 29-80). Most patients were immunosuppressed due to prior organ transplant (57/74, 77%). Seven (58%) AS patients underwent deferred treatment (6 ablations, 1 nephrectomy) due to progressive tumor growth. Surgical patients were significantly younger than ablation or AS patients and had fewer comorbidities. The surgery and ablation 30-day readmission rate (17% vs 9%, p=0.7) and 90-day complication rate (24% vs 21%, p=0.9) was similar, respectively. No 90-day deaths occurred. One (3%) surgical and 2 (6%) ablation patients recurred locally. One (3%) surgical, 1 (3%) ablation, and no AS patients progressed to metastatic disease. No significant differences were noted for the local recurrence free, metastasis free, and overall survival for the 3 cohorts (P>0.05 for all) (Figure 1). Conclusions: For medically immunosuppressed patients with cT1 RCC, treatment outcomes are similar to historical series of non-immunosuppressed patients. These data suggest that small RCC tumors are not more aggressive in patients with medical immunosuppression but require careful selection to avoid morbidity and maintain oncologic control. SOURCE OF Funding: None