MP17-06: Validation of EAU Risk groups for biochemical recurrence after radiotherapy and radical prostatectomy for prediction of prostate cancer mortality.
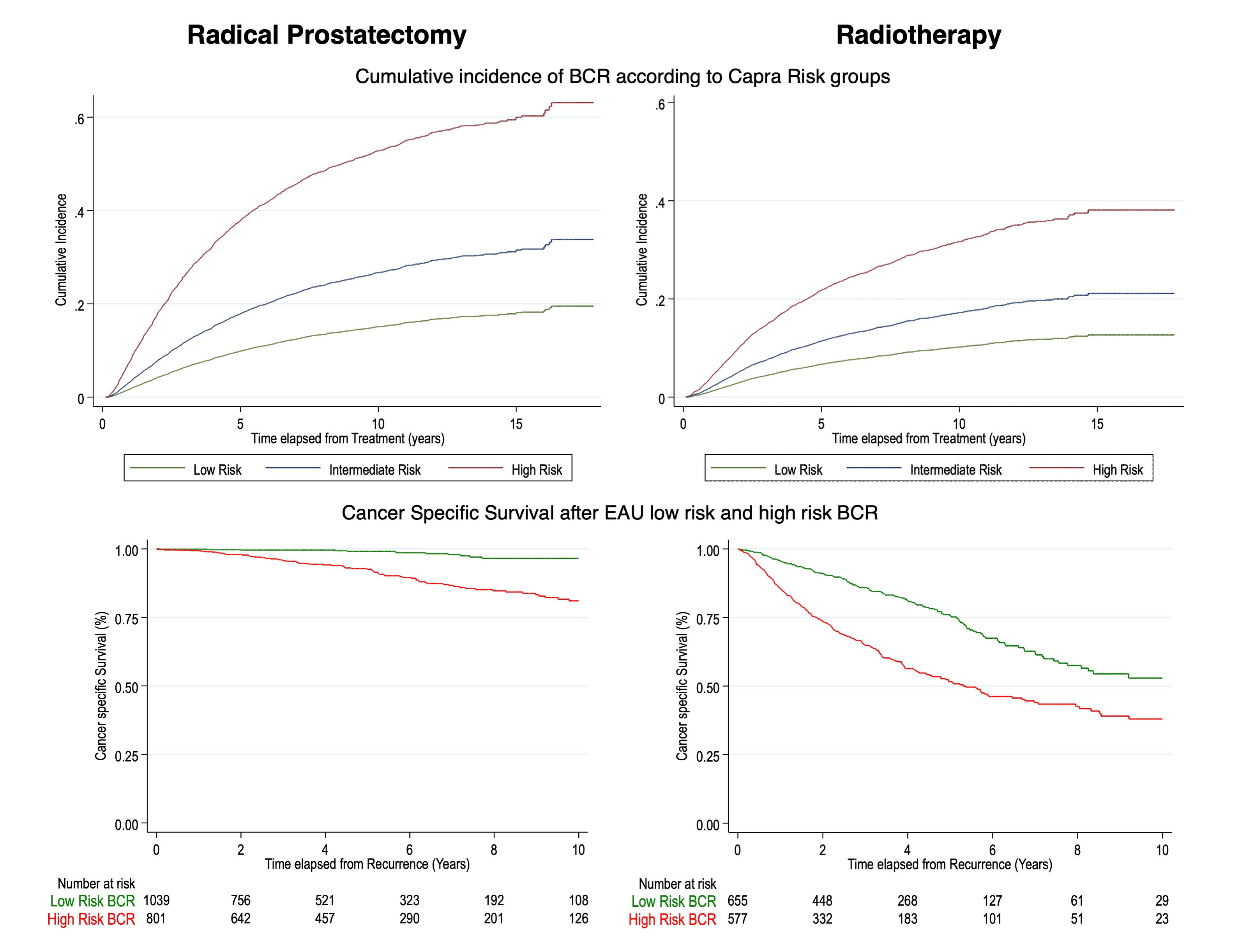
Introduction: EAU guidelines stratify patients with biochemical recurrence (BCR) after radiotherapy (RT) or radical prostatectomy (RP) for prostate cancer (PCa) in low risk (LR-BCR) and high risk (HR-BCR) based on biopsy ISUP Gleason group (bx GG), PSA doubling time (PSADT) and time to PSA recurrence. We aim to externally validate EAU-BCR risk groups by using long-term follow-up outcomes in a population-based study. Methods: We included all men in Stockholm County who underwent RT or RP with curative intent (localized PCa, cM0) and PSA follow-up from 2003 to 2019. PSA tests were performed in three centralized laboratories. BCR was defined as PSA=0.2 after RP and PSA nadir+2 after RT. Competing risk regression and multivariable variable Cox regression analysis were used to evaluate incidence of BCR according to CAPRA risk groups and the prognostic value of BCR risk groups on PCa specific survival (CSS) Results: 15 441 patients were included. Median follow-up length was 84 months (52, 129). In the RP group (n=9778), age-adjusted cumulative incidence of BCR at 15 years after RP was 20%, 35% and 60% in low, intermediate and high Capra risk. 1849 patients developed BCR and 801 (43%) had HR-BCR. CSS at 10 years after BCR was 96% and 75% for EAU LR and HR-BCR patients. In the RT group (n=5663), age-adjusted cumulative incidence of BCR at 15 years after RT was 15%, 22% and 38% in low, intermediate and high Capra risk. 1232 patients developed BCR and 577 (47%) had HR-BCR. CSS at 10 years after BCR was 51% and 38% for LR and HR-BCR patients. At multivariable cox regression adjusting for age and cT stage, individual covariates included in the EAU BCR risk stratification were found to be predictors of PCa mortality. Hazard ratios for HR-BCR compared to LR-BCR were 2.17 (CI 1.77,2.67) and 5.73 (CI 3.29,9.96) in the RT and RP groups. Conclusions: The cumulative incidence of BCR was higher after RP compared to RT patients but the risk of dying from PCa after BCR was higher after RT. EAU BCR risk groups help better stratify patients with a high risk of dying from PCa. However, while the risk of dying from PCa in LR-BCR after RP is very low, patients who develop an LR-BCR after RT have a high risk of PCa mortality. Current definitions of BCR after RP and RT and the EAU risk stratification are suboptimal to compare oncological outcomes after treatment for PCa. SOURCE OF Funding: This research was supported by a grant of the European Urological Scholarship Programme awarded to U.G.F.