Session: PD08: Kidney Cancer: Epidemiology & Evaluation/Staging/Surveillance I
PD08-05: Computer-Generated C-Index Nephrometry Scores Demonstrate Superior Predictive Accuracy to Those of Human-Generated Scores in Predicting Oncologic and Perioperative Outcomes
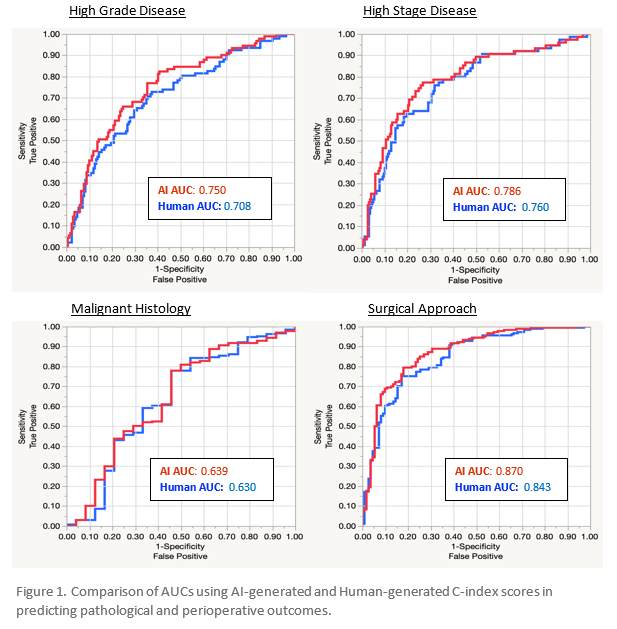
Introduction: The Centrality index (C-index) score is a nephrometry scoring system that requires precise measurements and mathematical calculations of cross sectional imaging. Its implementation has been slowed by requiring time investment and interobserver variability. We sought to automate this score on preoperative computerized tomography (CT) scans by developing an artificial intelligence (AI) generated C-index score (AI C-Index). Subsequently, we aimed to evaluate its ability to predict meaningful oncologic and perioperative outcomes as compared to human-generated C-index scores (Human C-Index). Methods: 300 patients with preoperative CT were identified from a cohort of 544 patients undergoing surgical extirpation for suspected renal cancer. A deep neural network approach was used to segment kidneys and tumors, and then programed to generate the measurements and calculate C-index score. Human C-index scores were calculated by medical personnel blinded to AI-scores. AI- and Human score agreement was assessed using linear regression and their predictive abilities for both oncologic and perioperative outcomes were assessed using logistic regression and compared with receiver operating characteristic (ROC) curve analyses. Results: Of 300 tumors, 27% were high stage (HS), 37% high grade (HG), 63% underwent partial nephrectomy, and median tumor size was 4.2 cm. There was significant agreement between Human and AI C-Index on linear regression (R2 = 0.738, p <0.0001). Both AI and Human C-Index similarly predicted oncologic outcomes, with lower levels of either score associated with increased risk of malignant histology (H-score p = 0.018, AI score p =0.014) HG disease (both p <0.0001), and HS disease (both p <0.0001). Lower levels of either score also predicted a radical nephrectomy rather than partial nephrectomy (both p <0.0001). AUC measurements (figure 1) were similar but consistently superior for AI C-index. Conclusions: Automated AI C-index scores are comparable to Human C-index scores and predict a wide variety of meaningful patient-centered outcomes. Our results suggest that our AI C-index could be delivered automatically from a preoperative CT scan to a clinician and patient at the point of care to aid in decision making. SOURCE OF Funding: None