Session: PD08: Kidney Cancer: Epidemiology & Evaluation/Staging/Surveillance I
PD08-08: Should Adjuvant Therapy be Considered for Positive Surgical Margins in Renal Cell Carcinoma: A Stage-Based Analysis of Impact of Positive Surgical Margins on Survival Outcomes Using the INMARC Registry
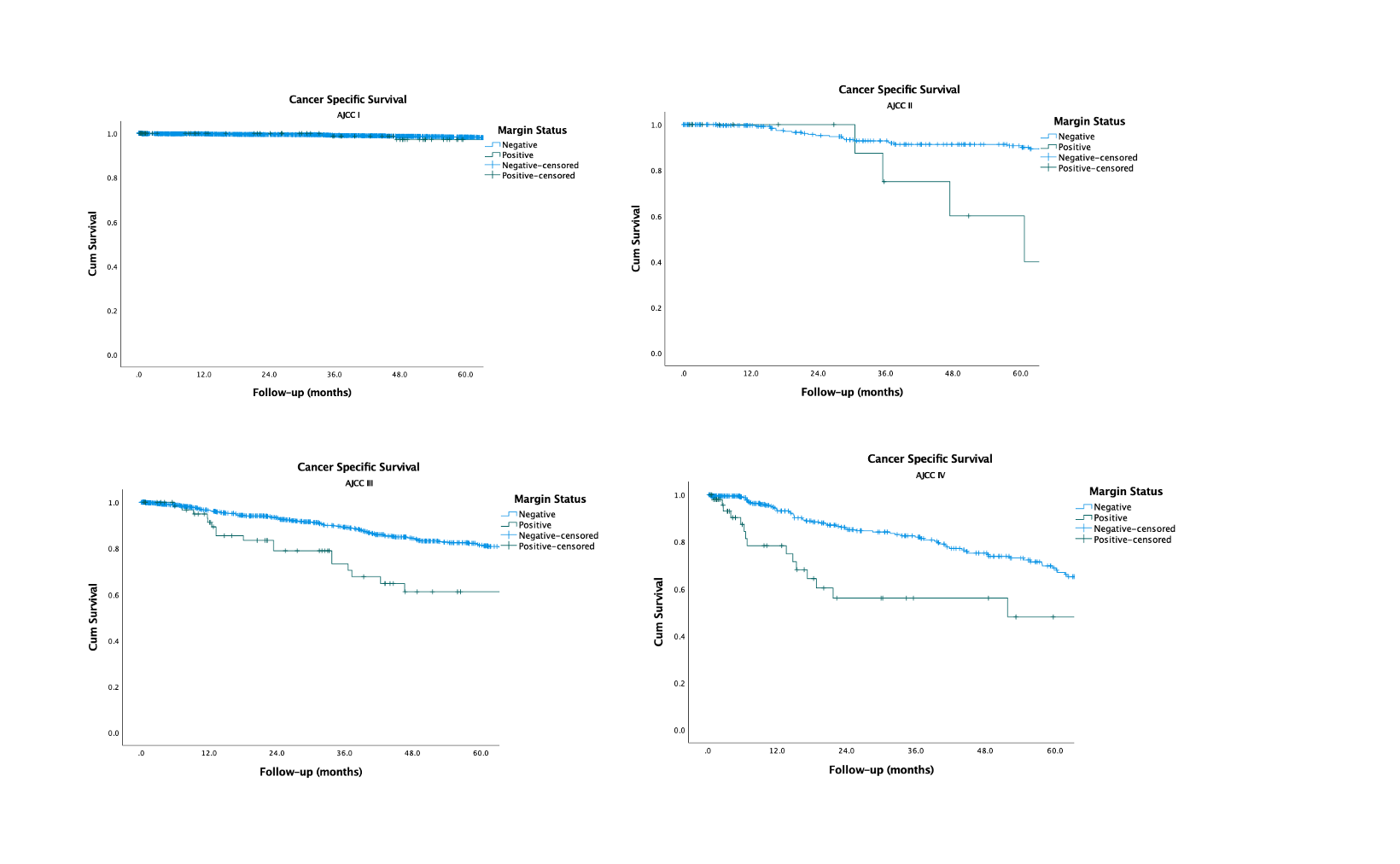
Introduction: Impact on survival by positive surgical margins (PSM) in Renal Cell Carcinoma (RCC) is controversial. While current guidelines recommend intensified follow up in PSM, no recommendations or investigation currently exist regarding adjuvant therapy and PSM. We sought to examine the impact of PSM on survival outcomes stratified by pathological AJCC (American Joint Commission on Cancer) Stage. Methods: Multi-institutional retrospective analysis of patients with RCC utilizing the INMARC (INternational Marker Consortium for Renal Cancer) registry who underwent surgery. Patients were divided by AJCC stage. Primary outcome was cancer specific mortality (CSM). Secondary outcomes included all cause mortality (ACM) and recurrence. Cox regression was utilized to analyze factors associated with outcomes. Kaplan Meier analysis (KMA) was performed to analyze 5-year cancer specific survival (CSS), overall survival (OS), and recurrence free survival (RFS). Results: 5112 patients were analyzed; PSM was present in 253 (114 stage I, 17 stage II, 71 stage III, 51 stage IV). Median follow-up was 49.3 months. Cox regression demonstrated that PSM was associated with worsened CSM (HR 2.1, p<0.001), ACM (HR 1.4, p=0.003), and recurrence (HR 2.1, p<0.001). KMA revealed significant differences in 5-year CSS by margin status across stage II (81% vs. 37%, p<0.001), stage III (82% vs. 61%, p<0.001), and stage IV (65% vs. 50%, p<0.001), but not stage I (99% v.s 98%, p=0.399). KMA revealed significant differences in 5-year OS by margin status across stage II (90% vs. 40%, p=0.003), stage III (67% vs. 41%, p<0.001), and stage IV (39% vs. 21%, p<0.001), but not stage I (87% vs. 91%, p=0.119). KMA revealed significant differences in 5-year RFS by margin status across stage I (97% vs. 83%, p=0.012), stage II (83% vs. 50%, p<0.001), stage III (64% vs. 59%, p<0.001), and stage IV (78% vs. 58%, p<0.001). Conclusions: Presence of PSM was an independent risk factor for worsened ACM, CSM, and recurrence in RCC patients and was associated with decrements in 5-year RFS across all stages and OS and CSS in Stage II-IV but not Stage I RCC. Our findings highlight the need for investigation of adjuvant therapy for stage =II RCC patients with PSM. SOURCE OF Funding: Stephen K Weissman Kidney Cancer Research Fund